This High Impact Change Model is a refresh of the existing Model and focuses on how the NHS and social care need to work together to avoid preventable stays in hospital. The primary focus is to reduce admissions to hospitals by remaining in or returning to the community.

Introduction: reducing preventable admissions
While sometimes hospital is the most appropriate place for someone to be, most people want to be at home and independent for as long possible, and generally this is the best place for them to recover. Emergency hospital care is the most expensive element of the NHS and, in a cost-constrained system, needs to be carefully managed.
Evidence has also highlighted that hospital admissions can expose people to a loss of independence and risk of infection, potentially reducing their health and wellbeing after leaving hospital. This can then lead to further demand on health services, and the expense of social care packages that may have been avoided through the right care in the right place initially.
This model aligns with current best practice and NHSE Neighbourhood health guidelines 2025/26. The best practice includes both helpful frameworks, and case studies with the latest examples and learning from across the country. The model aims to be practical, helping systems to more readily implement change and understand change enablers.
The model is centred around two goals:
- Goal 1: Prevent crisis: Actions to prevent crises developing or advancing into preventable admissions
- Goal 2: Stop crisis becoming an admission: Actions to divert or prevent an attendance at A&E becoming an admittance to hospital or long-term bed-based care.
The model contains:
- Top level overviews of key changes and outcomes
- Wider considerations for system leaders in leading these changes and putting them into practice
- Case studies of best practice and links to other useful resources
- Supplementary detail including practical tips, questions and watch-outs for considerations when implementing the changes
What has changed since the previous version?
The High Impact Change Model for ‘Reducing preventable admissions to hospital and long-term care’ was developed a number of years ago to provide best practice guidance and tools to health and care systems. Whilst it was updated to capture learning from the COVID-19 pandemic, this version brings it further up to date and aligns with the latest best practice – particularly the new approach to integrated neighbourhood health.
Key changes include:
- Making a clearer distinction between hospital and residential care admissions - while these are often related they are not the same. They often affect different cohorts and can be driven by different root causes, with many residential admissions coming straight from the community without an emergency health escalation. This model primarily focuses on hospital admissions and any secondary impact on social care demand. We acknowledge the same preventative approaches may have a positive impact for residential care admissions, but any transformation aiming to reduce residential admissions should tailor risk identification, intervention, and delivery model accordingly.
- An increased focus on prevention of crisis and proactive community-based interventions
- Additional content on building strong communities to complement empowering individuals to manage their health and wellbeing
- Consideration of key challenges and practical realities in implementing admission avoidance changes.
Overarching principles
There are eight principles that underpin this model and its implementation:
- Right care, right time, right place: Commitment and focus to support people to remain in their homes or usual place of residence, when they are having a health or social care crisis, preventing admission to hospital or long-term care where possible.
- After a crisis event, supporting people to maintain or regain skills, confidence and independence.
- Transferring power and knowledge to individuals and communities so they can take ownership of their health and wellbeing.
- The workforce understands the community it serves, and the individual is at the centre of all decision making.
- Inclusive, person-centred, strength-based partnerships with communities and individuals provide the foundation for reducing preventable admissions.
- Collaborate across partners to achieve impact at scale.
- Wider determinants of health and inequalities, as well as their compounding effects, must be considered and addressed in every high impact change.
- Use evidence about what works, draw on best practice, and then measure and iterate your local impact.
Model Overview - Top level overviews of key changes and outcomes: An Overview of the updated High Impact Change Model
The diagram below demonstrates the main elements of the High Impact Change Model. This is centred around three areas:
Identifying People At Risk: Effective use of Population Health Management to identify and support those at risk of a future hospital admission
An Integrated Neighbourhood Approach to Health and Care Services in preventing and responding to crises
Promoting Long Term Independence to help prevent future crises and reduce long term dependence on health and social care services
Each of the change areas A-G are expanded in the following section.
A: Identifying those most at risk of crisis
High Impact Change A: A person-level risk stratification model, driven by system-wide data insights, provides a shared and embedded view of admissions risk across multiple user groups.
B: Target and tailor interventions and support for those most at risk
High Impact Change B: Use quantitative and qualitative insights to co-design holistic, person-centred solutions, enabling flexible, integrated support that wraps around the person.
C: Neighbourhood MDTs coordination of complex cohorts
High Impact Change C: Establish multidisciplinary teams composed of professionals with the most relevant expertise, supported by efficient ways of working, clear accountabilities, and robust management systems to effectively manage caseloads across the system
D: Integrated community delivery
High Impact Change D: Deliver an integrated model of Community Services with right-sized capacity, underpinned by effective urgent response elements and streamlined emergency care pathways to ensure timely, coordinated support
E: Accessibility, flexibility and ease of navigation
High Impact Change E:Enhance general access and navigation through a flexible, resilient network of well-connected services that adapt to individual and system needs
F: Maximising independence and preventing future crisis
High Impact Change F: Implement services that empower individuals to maximise their independence, embed prevention into every contact, and proactively support high-risk cohorts through advance planning for future crises
G: Stronger community infrastructure
High Impact Change G: Drive system integration by aligning formal services and connected communities, enabling local areas to effectively coordinate action on admissions.
Putting this into practice: wider considerations for system leaders in leading these changes and putting them into practice
Clarity in what you are aiming to achieve
Craft a collective vision set out in a person-centred way, shared by all relevant parties, and which everyone is bought into and understands their role in achieving.
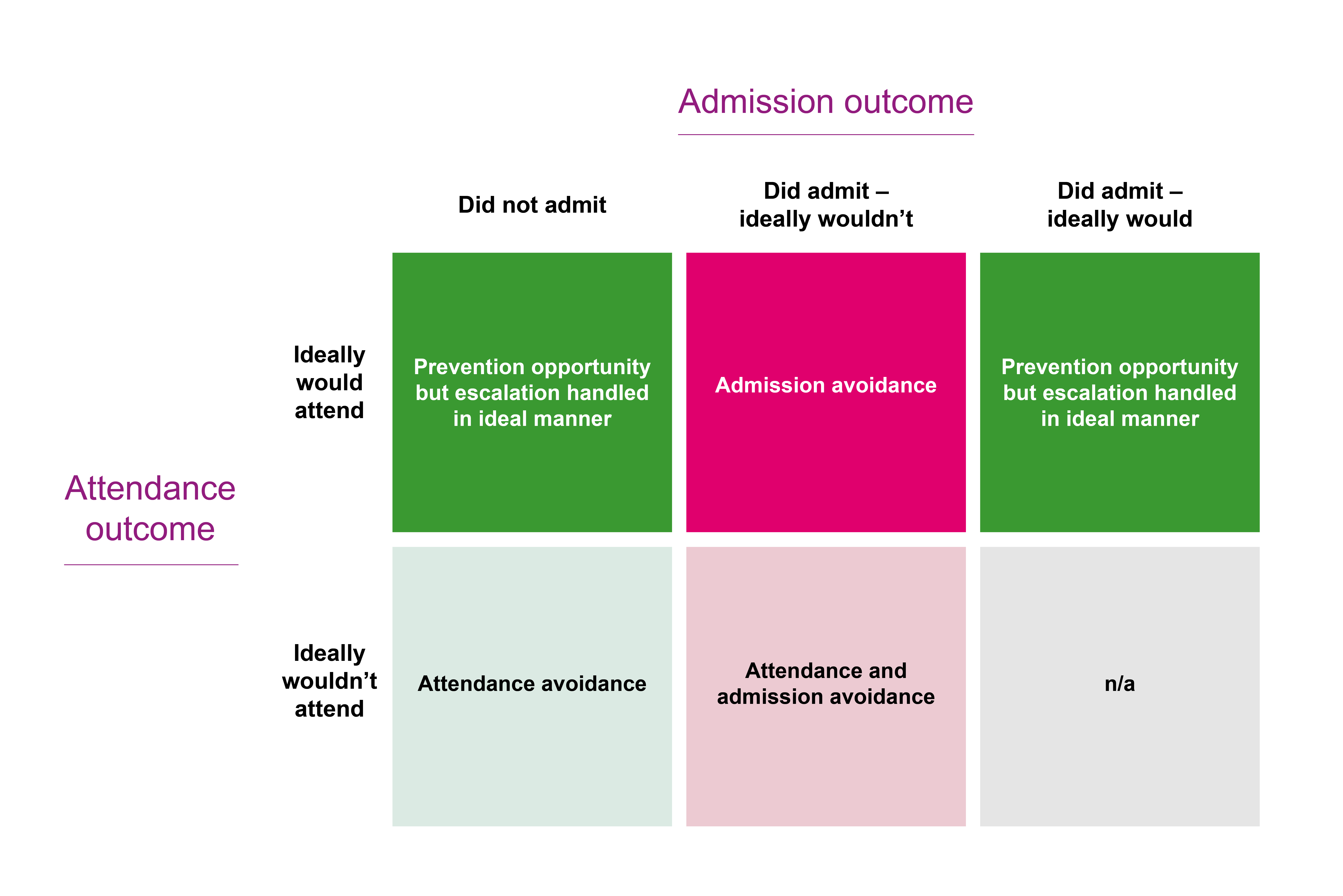
While there is an overlap between admission and attendance avoidance, depending on what the goals of the system are, the cohorts and pathways you focus on may be different. For example if reviewing acute ED Attendances, outcomes fall into the five boxes below. Each of these will have different volumes of people, but the specifics of their cases and what would have been ideal will be different in each case.
There may also be further opportunities beyond the acute hospital, for example reducing primary care demand, or improving ambulance response times.
To bring this to life with an example, if a Rapid Response Nursing Team finds a way to increase the number of people it can support by 10 per cent, should this be used to:
- Increase referrals from 111 and 999 pathways
- Increase referrals from paramedics
- Increase referrals from hospital to support people to return home.
In isolation all of these opportunities are valid, and it may be right to try and increase all three – but if you are trying to focus on admissions then each will impact this to a differing degree.
Knowing where to start
Each system has a unique starting position and often has several active schemes in population health management, prevention, and urgent response. As part of agreeing a single system approach, review the existing schemes’ potential impact and their scalability. Also consider other enabling factors such as digital requirements, substantive funding, and applicability across the variety of neighbourhoods in the system.
Conduct a thorough review of patient attendances and admissions to determine ideal outcomes. Identify necessary changes to current services or transformations, as well as existing gaps in provision or referral criteria.
Emphasise the significance of impact - a minor percentage improvement in a large population may be more beneficial in reducing acute bed demand than a more substantial percentage improvement in a smaller group of people.
Given limited resources and the need for prompt benefits, focus initially on high-risk groups with interventions aimed at preventing near-term escalations
Which activities should be managed by which organisation and at which geographic level?
Organisational roles
Consider whether you are making the most of all system partners including the VCFSE sector, and the role of acute teams in delivering care closer to home.
A key takeaway from neighbourhood health projects is that having one organisation act as an integrator is vital for assembling integrated teams and enhancing patient care.
Geographic scales
Local configurations must be considered, and while there isn't a universal solution, agreeing the roles and responsibilities is crucial. This will enable systems to tackle questions like infrastructure and digital assets, funding frameworks, and accountability clarity. They also need to find the right balance between local innovation and scalable system solutions.
Each scale comes with their own opportunities and challenges
- Role of Integrated Care Boards (ICBs): can set direction and build the frameworks for delivery and funding, but they have limited connection and leadership at a more local footprint level. They could aggregate skill-sets and capabilities like data science, financial evaluation, or programme management that would be sub-scale at a local level. They can also be an important conduit in sharing best practice and supporting scaling of models. As the role of ICBs evolves in the future, or their geographic footprints expand, these roles may also be found in provider collaboratives or accountable care organisations.
- Role of local authorities: often have strong links to their communities and care networks, but geographies are not always contiguous with health boundaries, and a large number of people who prevention could support are not directly in contact with social care, versus a significant majority already engage with NHS Services.
- Role of local leadership (for example, Primary Care Network or neighbourhood footprints) can drive energy, pace, and really tailor interventions to the local population. Primary care is often seen as a gateway by local people, and so plays a key role. NB This does not mean the local leader always needs to be a GP. There are risks in devolving completely to local areas, especially if aiming for a standardised model across a larger geography, how to find the balance between overfitting to a specific local footprint, versus building a scalable model applicable to knowledge share and roll-out across other footprints.
Measuring value across the system
Measuring the impact of prevention is challenging, but not impossible, and too often the challenge in measuring full system benefits prevents people measuring robustly within schemes at a more micro level.
Within initiatives the operational KPIs should be recorded and used to estimate potential impact – e.g. number of people supported, types and volumes of interventions, outcomes for the people on the caseload. This can be supplemented by qualitative evidence as to the experience for the individuals supported.
Systems require pragmatic approaches to trace benefit from changes in the community all the way through to the acute hospital impact – and a good understanding the various potential forces at play:
- Natural variation in acute activity when looking at very small geographies and conditions identified as preventable – this becomes much easier at scale
- General baselines of rising attendances and admissions mean preventative activity may be acting as demand avoidance rather than a cash-releasing bed reduction opportunity
- Pressures on acute bed bases mean initial improvements may be absorbed by e.g. reductions in occupancy, or clearing of queues in an emergency department – these are inherently valuable activities, but have less direct relation to the acute hospital budget
To fully evaluate collective prevention efforts require more complex statistical analysis. The practical effort for any one scheme is probably best invested in creating a clear logical link from activity taking place in the community and the estimated impact on acute activity. These estimates can be tested and refined as trials progress. Those who are identified as at risk but decline an intervention can have their outcomes tracked as a control group.
Keeping pace with future developments
At the time of writing, the NHS and local authorities are undergoing significant structural change with the abolition of NHSE and reduction in size of ICBs, coupled with the direction towards unitary authorities. This will impact the roles and responsibilities in a system to set up and deliver preventative and admission avoidance initiatives.
This model focuses on avoiding hospital admission and the resultant days spent in a hospital bed. However there are wider potential benefits for health and social care. Each organisation would also be able to identify further activity they would ideally prevent too. Combining resources and integrating via local neighbourhood teams gives a great opportunity for this prevention agenda, but it may not be possible to aggregate and achieve all organisational priorities simultaneously. Agreeing roles, priorities and incentives across organisations is key.
We can also expect there to be workforce evolution – with the development of more hybrid roles in particular. Case management is one example of a skill that can be applied across a number of roles in community care, and it’s possible that going forwards there are more clinical or care skills that also become shared, or career pathways that encourage people to move across disciplines and build a more holistic skill set.