The High Impact Change Model (HICM) for Optimal Handed Care (OHC) provides a practical framework to embed OHC in different care settings across health and care systems. It aims to ensure that every person receives safe, proportionate, and independence-focused care and support, while reducing workforce strain and maximising system efficiency.

Over 60 stakeholders have participated in developing this high impact change model, including people receiving care, carers, clinicians, professionals, other front-line staff and policymakers. The model reflects stakeholders’ voices and their preference for developing a model that focuses on the practicalities and what needs to happen on the ground. The Royal College of Occupational Therapists (RCOT) has officially endorsed this HICM.
Optimal Handed care (OHC), also referred to as proportionate care, single-handed care, right-sized care, optimised care or optimised handling, is defined as a “A comprehensive assessment of an individual’s ability to safely engage in daily activities, making use of assistive equipment where appropriate, with the expectation that care will be delivered in the most proportionate and efficient way possible.” In this document ‘Optimal Handed Care (OHC)’ has been used as an umbrella term for all the above.
Why change is needed
Unsafe or disproportionate moving and handling practices increase dependency, cause staff injury, and drive unsustainable costs across the system. Despite existing policy and training, variation in practice persists between organisations and sectors.
Current challenges and their impact on people and the workforce / system
Getting Optimal Handed Care right presents a significant opportunity for systems to both improve care quality and efficiency. Pockets of good practice already exist that have produced compelling outcomes. Yet, so far these are mainly bottom-up, small scale initiatives which can sometimes falter due to lack of senior leadership.
To seize the opportunity at scale, a radical shift of emphasis is needed, owned by system leaders who can drive the work to gather evidence, understand the extent of the problem and quantify the opportunity in their systems. Leaders need to make this topic their business.
Vision
A fully integrated, person-centred model in which Optimal Handed Care becomes standard practice — delivering the right level of support, by the right number of carers, at the right time. A shared responsibility of all partners in the system to ensure people are supported to be as independent for as long as possible.
High Impact Change Areas
At-scale implementation requires a systematic and phased approach across the system to ensure OHC is embedded across all care settings. It requires health and care systems to first build the foundations, pilot, gather evidence, followed by phased implementation across the system ensuring all stakeholders remain fully engaged.
Consideration of ‘high impact areas’ reflects the learning, operational experience and good practice established through extensive engagement of over 60 stakeholders including people with lived experience, senior clinicians, front line practitioners, managers and senior policy makers, highlighting the need for cultural shift in the hospitals and systematic support in the community.
The diagram and table below show the steps involved in bringing this to life with eight high impact change areas as outlined below.
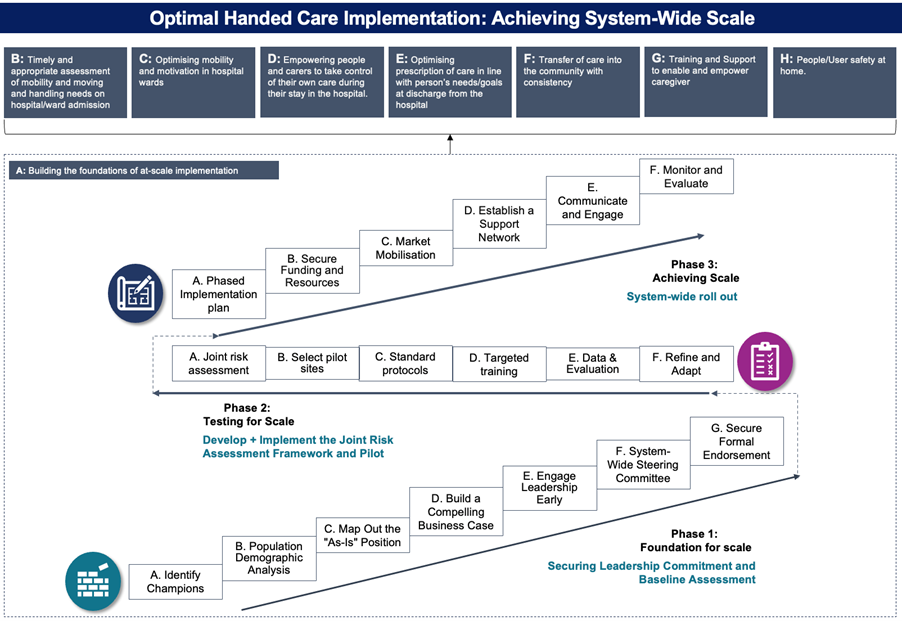
FIGURE 1: Optimal Handed Care implementation: Achieving system-wide scale
Please note that the diagram tracks a person’s journey from acute into the community, however, in practice it can start in any care setting. Indeed, social care has a long history of Optimal Handed Care and are often well-placed to provide leadership and training to all system partners.
A. Building the foundations of at scale implementation
- Focus: Establish strong, accountable system leadership; shared governance; clear OHC vision
- Intended impact: Creates sustainable culture, consistent standards, and clear accountability for OHC delivery.
B. Timely and appropriate assessment of function, mobility and moving and handling needs on hospital / ward admission
- Focus: Embed standardised assessment tools; ensure early identification of functional ability, mobility and OHC needs; integrate assessment data into electronic records.
- Intended impact: Reduces deconditioning and delayed discharges; ensures people’s needs are understood early and addressed safely.
C. Optimising mobility and motivation in hospital wards
- Focus: Foster active recovery culture; empower people to maintain mobility; train staff to encourage independence
- Intended impact: Improves physical outcomes, reduces dependency, and supports early rehabilitation and discharge.
D. Empowering people and carers / representatives to take control of their own care during hospital stay
- Focus: Promote co-production and self-management; provide education and equipment training; involve families in care planning and mobility goals.
- Intended impact: Enhances confidence, self-efficacy, and continuity of care; strengthens patient and carer engagement.
E. Optimising provision of care in line with a person’s needs and goals at discharge from hospital
- Focus: Align discharge planning with OHC principles; communicate expectations clearly; adopt proportionate language and assessment-based care packages.
- Intended impact: Ensures proportionate, needs-led discharge; supports recovery at home and reduces dependency.
F. Transfer of care into the community with consistency
- Focus: Create seamless pathways from hospital to home; strengthen occupational therapists (OT)–Social Work collaboration; enable rapid response and reablement follow-up.
- Intended impact: Ensures continuity of OHC in the community; prevents duplication, care escalation, and readmission
G. Training and support to enable and empower caregivers (family/friends) to provide optimal care
- Focus: Deliver structured OHC training; embed mentoring and review visits; promote confidence and safe handling for informal and paid carers.
- Intended impact: Improves safety and wellbeing for carers; supports sustained independence and optimised care at home.
H. People/user safety at home
- Focus: Ensure safe environments through appropriate equipment, home assessments, and environmental adaptations; embed telecare and review mechanisms.
- Intended impact: Reduces accidents and injuries; maintains independence and dignity in the home environment
Case studies
- The implementation of proportionate care (or optimal handling care) at University Hospital Southampton
- The implementation of Optimal Handed Care in Kirklees Council
- The implementation of Optimal Handed Care across Manchester City Council
- Optimisation of function and mobility at North Cambridgeshire Hospital
- The British Red Cross: Train the Trainer; Moving and Handling
The successful implementation of the HICM is expected to deliver significant improvements across health and care systems.
Achieving these benefits requires:
- strong, collaborative leadership commitment and accountability across all Health and care system partners
- a collaborative culture that involves people in their care decisions, empowering them to make informed choices about their care
- value based, integrated and function focused commissioning at a system level instead of traditional organisational and service-based commissioning
- comprehensive training programmes for all assessors and caregivers (formal and informal) across the system
- system wide consistent escalation approach with a timely response to ensure care provision always remains optimised
- continuous monitoring and evaluation of outcomes for people, staff and health and care system to drive improvement and ensure consistency in approach, practice and equipment provision across the system.
By focusing on people’s independence, system-wide collaboration, and a commitment to continuous improvement, health and care systems can embed Optimal Handed Care across all care setting and create a more sustainable, efficient, and person-centred health and care system.
Expected outcomes
People and System Transformation through OHC
Successful implementation of the High Impact Change Model (HICM) for Optimal Handed Care (OHC) has the potential to create radical, transformative changes for both the population and the broader health and care system. By prioritising individual needs, fostering collaboration, and focusing on continuous improvement, OHC leads to more effective, efficient, and sustainable care.
Acknowledgements
The development of the High Impact Change Model for Optimal Handed Care (OHC) has been made possible through the insight, expertise and generosity of professionals, providers, people with lived experience, and partners across the health and social care system.
We extend our sincere thanks to everyone who contributed their time, evidence and perspectives during the creation of this national model.