
Executive summary
“We all want to live in the place we call home, with the people and things that we love, in communities where we look out for one another, doing the things that matter to us”
Participation in activities of everyday life – occupations – matters. It is essential to our health and wellbeing; it gives us a sense of purpose and meaning – our identity; it is a right of all people, regardless of their abilities, recognised by the United Nations.
Occupational therapists (OTs) enable barriers to participation in activities of everyday life to be overcome, working with people of all ages, with physical and mental health needs, and those who support them.
As a science-based, clinical and registered profession for over 100 years, Occupational therapists (OTs) epitomise person-centred care by focusing on strengths, hopes, and aspirations beyond diagnoses and limitations. This approach enables better outcomes and independence for individuals. Their expertise extends beyond healthcare to address broader health inequalities, promote prevention, and support individuals in achieving independence. As outlined in the report under ‘Improving and protecting the public’s health’, this includes contributions to public health, inclusive housing and reducing inequalities.”
Despite the significant role of OTs, councils have not been sufficiently and sustainably resourced to deliver the Care Act 2014. If they had been, many more OTs would likely be working in the community today, benefiting a larger number of people and communities. As evidenced in the ‘Enabling the things that matter to us: the role in prevention in the Care Act 2014 context’ section, occupational therapists support Care Act duties and enable better outcomes through prevention and early intervention.”
OTs in councils work primarily in adult social care or housing, reflecting statutory duties. They are already contributing to delivering key priorities for communities and the Government’s missions. However, the Local Government Association (LGA) believes there is unrealised potential. This is particularly significant as the Government seeks to enhance public health, facilitate employment and skills development, and deliver health and care services within communities to ease NHS pressures. OTs’ contributions to future-proofing home environments, the shift to neighbourhood care and the Government’s ambitious housebuilding agenda, make them essential to achieving these national goals.
To explore this potential, the LGA commissioned research, in collaboration with the national Principal and Strategic Occupational Therapists Network, the Royal College of Occupational Therapists, Foundations, and others, to explore this potential. The research focuses on adult services and describes the basis for OTs' contributions to prevention in the context of the Care Act 2014, protecting and improving public health, and enabling healthy, suitable homes and jobs. The research outlines why these contributions matter and what more OTs could do. Detailed discussion can be found in the evidence sections ‘Preventing, delaying and reducing the need for care and support’, ‘Improving and protecting the public’s health’ and ‘Inclusive growth: everyone is better off’, which together highlight the occupational therapy role in prevention, public health and inclusive growth. The report also highlights the critical role OTs play in health and care integration, ensuring that services are delivered seamlessly across sectors by professionals who understand both systems.
Local authorities are under huge financial pressure. It is increasingly difficult to support OTs’ professional development, attract new talent, or retain existing staff—despite their importance to statutory delivery and service transformation.
The LGA’s asks of the Government for councils after conducting this research include:
- Provide financial stability and parity: Ensure pay and working conditions for council-employed OTs match their NHS counterparts by providing councils with the necessary funding and flexibility to do so. Councils need resources to recruit, train and retain a sustainable workforce.
- Focus on prevention: To reform and sustainably fund adult social care to give councils the opportunity to properly invest in prevention.
- Unlock OT potential: Take specific actions to realise the potential of OTs in councils, enabling them to contribute more effectively to the health and care system in both the short and longer term.
This report is part of a broader conversation on prevention and the integration of health-funded professionals into local government. The LGA remains committed to advancing this agenda in partnership with national and local stakeholders. By addressing these asks, the Government can help unlock the full potential of councils and their work forces delivering better outcomes for people, easing pressure on health services, and strengthening communities.
Recommendations for Government
These recommendations are based on the findings of this research and the experiences shared by occupational therapists working in councils. They reflect where targeted government action could unlock the full potential of OTs to deliver better outcomes, support statutory duties, and strengthen community-based care.
1. Recognise the value of occupational therapy
Occupational therapists play a vital role in preventing, delaying, and reducing the need for care and support, contributing significantly to positive outcomes for individuals, communities, and neighbourhoods. as evidenced in the ‘Enabling the things that matter to us’ section, OTs support Care Act duties and enable better outcomes through prevention and person-centred care. Their work supports the delivery of local authority statutory duties and health and social care reform. Embedding an OT adviser with responsibility for local authorities in the Department of Health and Social Care would further promote OT leadership and practice and a encourage a stronger shift towards prevention across councils.
2. Invest in sustainable funding
Councils require additional and consistent financial resources to deliver the Care Act effectively. This includes multi-year settlements and non-ringfenced grants that allow flexibility to sustain services. Ensuring pay and conditions for OTs are on par with NHS counterparts is essential to workforce retention and service sustainability. The ‘Occupational therapists in councils: the workforce’ section outlines how funding constraints affect recruitment, retention, and parity with NHS-employed OTs.
3. Address the shortage of occupational therapists
As discussed in the ‘Occupational therapists in councils: the workforce’ section, workforce shortages and lack of career progression are key barriers to service delivery. National workforce development strategies must focus on increasing OT numbers and creating opportunities for professional learning and career progression. Developing integrated, person-centred care pathways with NHS and other partners will reduce duplication of effort and enhance the impact of OTs.
4. Improve data and evidence collection
Better data on the contributions and outcomes of OTs is needed to showcase their value and optimise their role within local health and care systems. The ‘Enabling the things that matter to us’ section highlights how current systems fail to capture OT contributions, limiting visibility and strategic planning. National consistency in data would help identify areas for improvement and support the case for further investment.
5. Address barriers in the Disabled Facilities Grant
The means-tested nature of the Disabled Facilities Grant limits access for working-age populations who would benefit from adaptations to support their independence. Reforming the grant would enable broader access and improve outcomes for those in need. The ‘The place we call home: enabling healthy, safe and suitable environments’ section explores how the means-tested nature of the DFG restricts access for working-age adults.
6. Support research and innovation
Investment in research is needed to further understand the impact of prevention and the contributions of OTs, particularly for individuals with complex needs. Tools to support population health approaches would help identify where OT services are most needed and maximise their impact. The evidence sections ‘Preventing, delaying and reducing the need for care and support’, ‘The place we call home: enabling healthy, safe and suitable environments’ and ‘Inclusive growth: everyone is better off’ all call for more evidence on OT impact, particularly in prevention, housing, and employment.
Recommendations for Health and Care Partners (e.g., NHS)
These recommendations are drawn from the findings of this research and the insights shared by occupational therapists working in councils. They reflect where health and care partners can play a vital role in enabling OTs to contribute more fully to integrated, person-centred care
1. Foster collaboration between councils, the NHS, and the voluntary sector
Partnerships are essential to optimising the contribution of OTs and reducing duplication of effort. Joint frameworks would enable professionals to work seamlessly across organisational boundaries.
2. Invest in sustainable workforce models
Health partners should work alongside councils to develop integrated, person-centred workforce strategies that explicitly references OT. Parity in pay and conditions between NHS and local authority-employed OTs is critical to maintaining a strong and stable workforce.
3. Include OTs in public health strategies
OTs should be integral to designing and delivering prevention-focused health initiatives. Their expertise in promoting wellbeing and independence can significantly enhance outcomes for individuals and communities.
4. Enhance data collection and research
Improved local datasets are needed to understand the full impact of OT contributions. Research into innovative OT practices, particularly for those with complex needs, will provide a stronger evidence base for future investment.
5. Promote OT leadership
Health partners should ensure that OTs are included in strategic decision-making and leadership roles within integrated care systems. This would support more effective collaboration and improve service delivery across sectors and support delivery of system clinical and care professional leadership ambitions - Clinical and care professional leadership in integrated care systems.
Introduction
The Local Government Association (LGA) is a cross-party local authority membership organisation, working on behalf of councils in England to ensure local government has a strong, credible voice with national government. This document is intended for stakeholders in England, including government departments, local authorities, and health and care organisations. It aims to influence and set the political agenda on issues that matter to councils, so they can deliver local solutions to national problems.
Purpose and scope
The LGA commissioned this research to explore how central government can better support occupational therapy (OT) services within councils and recommend actions that the LGA or others could take to enable this. The focus is on adult services and the Government’s missions for the NHS and economic growth.
Intended audience
This document is specifically tailored for stakeholders in England, including:
- Government departments: To inform policy and funding decisions.
- Local authorities: To guide the implementation and optimisation of OT services.
- Health and care organisations: To support collaborative efforts in improving public health and social care outcomes.
Background
Occupational therapy has existed for over 100 years as a science-based, clinical, and registered profession. Occupational therapists (OTs) epitomise person-centred care by focusing on strengths, hopes, and aspirations beyond diagnoses and limitations. This approach enables better outcomes and independence for individuals.
Despite the significant role of OTs, councils have not been sufficiently and sustainably resourced to deliver the Care Act 2014. If they had been, many more OTs would likely be working in the community today, benefiting a larger number of people and communities.
There are around 43,500 registered OTs. Most OTs are employed by the NHS. 3,200 are employed by councils, primarily in adult social care or housing, reflecting statutory duties. Under Section 75 arrangements some OTs delivering the local authority and housing role are employed by the NHS. These OTs already contribute to delivering key priorities for communities and the Government’s missions. However, the LGA believes there is unrealised potential.
The LGA commissioned research, with input from the national Principal and Strategic Occupational Therapists Network, the Royal College of Occupational Therapists, Foundations, and others, to explore this potential. The research focuses on adult services and Government missions for the NHS and economic growth. It describes the basis for OTs' contributions to prevention in the context of the Care Act 2014, protecting and improving public health, and enabling healthy, suitable homes and jobs. The research outlines why these contributions matter and what more OTs could do.
Challenges facing councils
An ageing population and more complex needs for care and support are placing immense pressure on councils. The cost of provision is also rising. The Association of Directors of Adult Social Services (ADASS) reports that £914 million of additional funding is needed in 2024/25 to meet the same level of need as the previous financial year. Directors estimate that just over £800 million of the demographic pressure will be funded, with the cost of the remainder having to be met through cuts to other services or use of other funding.
Workforce challenges also present a significant issue in understanding, assessing, and meeting care and support needs in a timely way. There are waiting lists for assessments of care packages and home adaptations, for care packages to commence or direct payments, or care plan reviews. Unmet and under-met needs have an impact on people and communities, on professionals, their services, and organisations. While waiting for care and support, the needs of individuals, their carers, and others in their support networks can escalate.
Councils and Directors of Adult Social Services (DASS) want to focus on prevention and are asking the government to work with them to enable this:
- According to the ADASS Spring Survey, 63 per cent of DASS feel less than confident that they have a sufficient budget to meet their legal prevention and wellbeing duties in 2025/26; less than 7 per cent of the adult social care budget is invested in prevention in 2024/25, a year-on-year decrease.
- If the Better Care Fund did not require such a focus on hospital discharge, ‘community prevention and early support services’ would be the priority.
- Should there be sufficient and sustainable resources, there are significant opportunities for improvement in information, advice, and advocacy for people who are not yet known to the council but are thinking about the future.
Framework for Prevention in Social Care and Occupational Therapy
The vision of the Care Act 2014 was for a care and support system that actively promotes wellbeing and independence, requiring local authorities to:
- Provide or arrange for services to prevent, delay, or reduce care needs.
- Identify the prevention services, facilities, and resources already available.
- Promote diversity and quality of services so customers have a choice of service.
Statutory guidance accompanying the Act acknowledges that occupational therapists ‘are effective at preventing, reducing, or delaying needs for care and support’ and are ‘likely to have a holistic picture…including consideration of a person’s strengths and informal support networks’.
The Act and statutory guidance:
- Introduced prevention responsibilities applicable to people who do not have any current needs for care and support, adults with needs for care and support, whether their needs are eligible and/or met by the local authority or not, and carers.
- Did not provide a single definition of prevention, recognising many different types of support, services, facilities, and other resources contribute.
- Suggested that the focus of prevention should be on wellbeing: understanding and enabling care and support needs to be met in the context of a person’s skills, ambitions, and priorities; developing resilience and promoting individual strength.
The Act paved the way for a shift from service-led offers of care and support to offers based on a key question in working with people: ‘What does a good life look like for you and how can we work together?’ Since the emergence of the profession in the 1910s in the UK, this way of working with people has been at the heart of occupational therapy.
Care Act 2014 statutory guidance describes three levels of prevention:
- Universal/Primary Prevention: Accessible to people with no current health or care and support needs, to promote wellbeing and avoid crisis.
- Targeted/Secondary Prevention: Accessible to people with an increased risk of developing needs, to intervene early, to slow down or reduce further deterioration.
- Specialist/Tertiary Prevention: Accessible to people with established or complex conditions, to minimise effects of disability or deterioration, to regain skills and manage, to reduce need where possible.
Workforce data and challenges
Available data about the workforce is limited and considered insufficient to enable local health and care systems and employers to plan for, and meet, their populations’ needs effectively. The Royal College of Occupational Therapists (RCOT) has long campaigned for this to be addressed and continues to seek improvements in intelligence through its new Workforce Strategy.
Analysis of currently available data by RCOT suggests that most of the workforce is employed in the NHS, but notes that some of the disparity between the number of OTs registered with the Health and Care Professions Council and those working in the NHS or for a council is likely due to an increasing number of OTs working independently.
Occupational Therapist workforce by employer:
| Employer | Total |
|---|---|
| NHS England – total (NHS workforce data, on the number of therapists employed by NHS providers, covers the whole of the NHS occupational therapy workforce, including assistants and support workers. NHSE figures are for whole time equivalents and cover just England.) | 21,454 |
| Acute trust | 10,430 |
| Care trust | 188 |
| Community trust | 1,949 |
| Mental health trusts | 8,075 |
| Other | 780 |
| National Health Service (Primary Care) | 200 |
| Non-NHS | |
| Local authority social services | 3,200 |
| Other: Independent Practice Voluntary and Community Sector Work rehabilitation services Universities Education |
There is limited information collected on the workforce outside of the NHS and local government. OTs counted here (and in the NHS) may be contracted to provide services to a council |
| UK HCPC registered OTs (HCPC, the statutory regulatory body for occupational therapists, provides raw data on the number of registered occupational therapists; figures are a headcount and cover the UK. OTs will be delivering adult’s, children’s and young people’s services, and in a range of sector settings: in the NHS, in the independent and other sectors. The published registration data does not pick up on these distinctions. These figures only provide a partial picture of the workforce, excluding non-registered therapy staff such as therapy assistants.) | 43,495 |
Sources: RCOT, NHS Digital, 2023. Primary Care Network Workforce and Skills for Care, 2023.
2022/23 Skills for Care estimated data on the adult social care workforce, and registered occupational therapists within this suggests:
- The number working in councils (3,200) has not changed since 2020, having risen from 2,700 since 2016. This is in the context of an increasing emphasis on prevention in health and social care, including the Discharge to Assess (D2A) model, and NHS Intermediate Care Framework.
- There is a lack of confidence in this figure. Whilst it should be noted some OTs delivering local authority statutory functions are employed by the NHS under Section 75 arrangements the overall numbers are low compared to those delivering NHS responsibilities.
- The vacancy rate for OTs working in councils has increased to 9.5 per cent from 6.8 per cent in 2020/21, comparable with registered social workers. Councils had 375 occupational therapist vacant posts (450 for all adult social care roles).
- The average number of sick days is 7.9 days, the third highest in the workforce. Workers with high sickness rates were more likely to leave. Staff turnover for OTs in councils is estimated to be 13.6 per cent.
- Most OTs (90 per cent) are female, the highest percentage of all professions in the adult social care workforce.
- OTs are among the least ethnically diverse job roles: 83 per cent are White.
- The mean age is 44.7 years, and the average number of years’ experience in the sector is 11.2 years.
Role of Allied Health Professionals (AHPs)
OTs are one of 14 Allied Health Professions (AHPs), working across the spectrum of health and care, education (including early years), academia, research, criminal justice system, voluntary, and private sectors. They are the third largest clinical workforce in the NHS (185,000 people), but they are the smallest registered professional group in social care. NHS England has a Chief Allied Health Professional who leads the development and delivery of the AHP Strategy for England, 'AHPs Deliver.'
This context is important for councils. While there are almost 43,500 OTs registered with the Health and Care Professions Council, there are just 3,200 OTs employed by councils.
Structure of the report
The report is structured to provide a comprehensive overview of the role of OTs in councils, the challenges they face, and the recommendations for optimising their contributions. It includes:
- Why occupation matters: An exploration of the importance of occupational therapy and the role of OTs.
- The difference OTs can make: Detailed sections on how OTs contribute to preventing, delaying, and reducing the need for care and support, improving public health, and promoting inclusive growth.
- Workforce challenges and recommendations: An analysis of the current workforce challenges and specific recommendations for addressing these issues.
- Case studies: Examples of successful OT initiatives in councils to illustrate the impact and benefits of OT involvement.
By addressing these areas, the report aims to provide a clear and actionable roadmap for enhancing the role of occupational therapists in councils, ultimately benefiting more people and communities.
Why occupation matters and what occupational therapists do
‘We all want to live in the place we call home, with the people and things that we love, in communities where we look out for one another, doing the things that matter to us.’
Activities of everyday life – occupations - are essential to our health and wellbeing. The roles we play, our habits and routines, values and beliefs, give us a sense of purpose and meaning – an identity.
Occupational therapists (OTs) work with individuals (and those who support them) to enable participation in activities. It is a science-based, clinical and registered profession. Practitioners are dual trained, working with people with physical and mental health needs, and are required to ensure that their practice meets standards required, through undertaking continuous professional development.
Occupations
The right of all people, regardless of their abilities, to have opportunities to participate in a full range of everyday activities within their community is recognised by the United Nations. This right underpins the concept of occupational therapy philosophy and practice.
An occupation is any activity that we need, want or like to do to live, throughout life, to look after our physical and mental health, and emotional and spiritual wellbeing, from the moment we’re born. Activities include self-care, such as washing, eating or sleeping; productive activities, such as work, study, caring or domestic activities, and leisure, such as playing sports, hobbies or socialising.
We’re all unique and so are the occupations that matter to us. They give our lives meaning, purpose and structure, and help shape who we are, connect us to others and help create our identity and sense of belonging. Through occupation we enhance our health and quality of life.
Occupations change throughout our life and are particularly important when we’re going through times of change. When can no longer do an activity, or need to adjust how we do it, our sense of self and purpose may change.
Occupational therapy
The occupational therapy profession has existed for over 100 years, yet the role of occupational therapists isn’t well understood by those outside the profession.
“You don’t know you need an occupational therapist until you need an occupational therapist.”
Quote from a carer
The primary goal of occupational therapy is to enable people to participate in the activities of everyday life. Occupational therapists help people of all ages overcome challenges completing everyday activities, see beyond diagnoses and limitations to hopes and aspirations, and look at relationships between the activities, alongside the challenges faced and the environment.
The person, environment and occupation model: OTs enabling participation in everyday activities
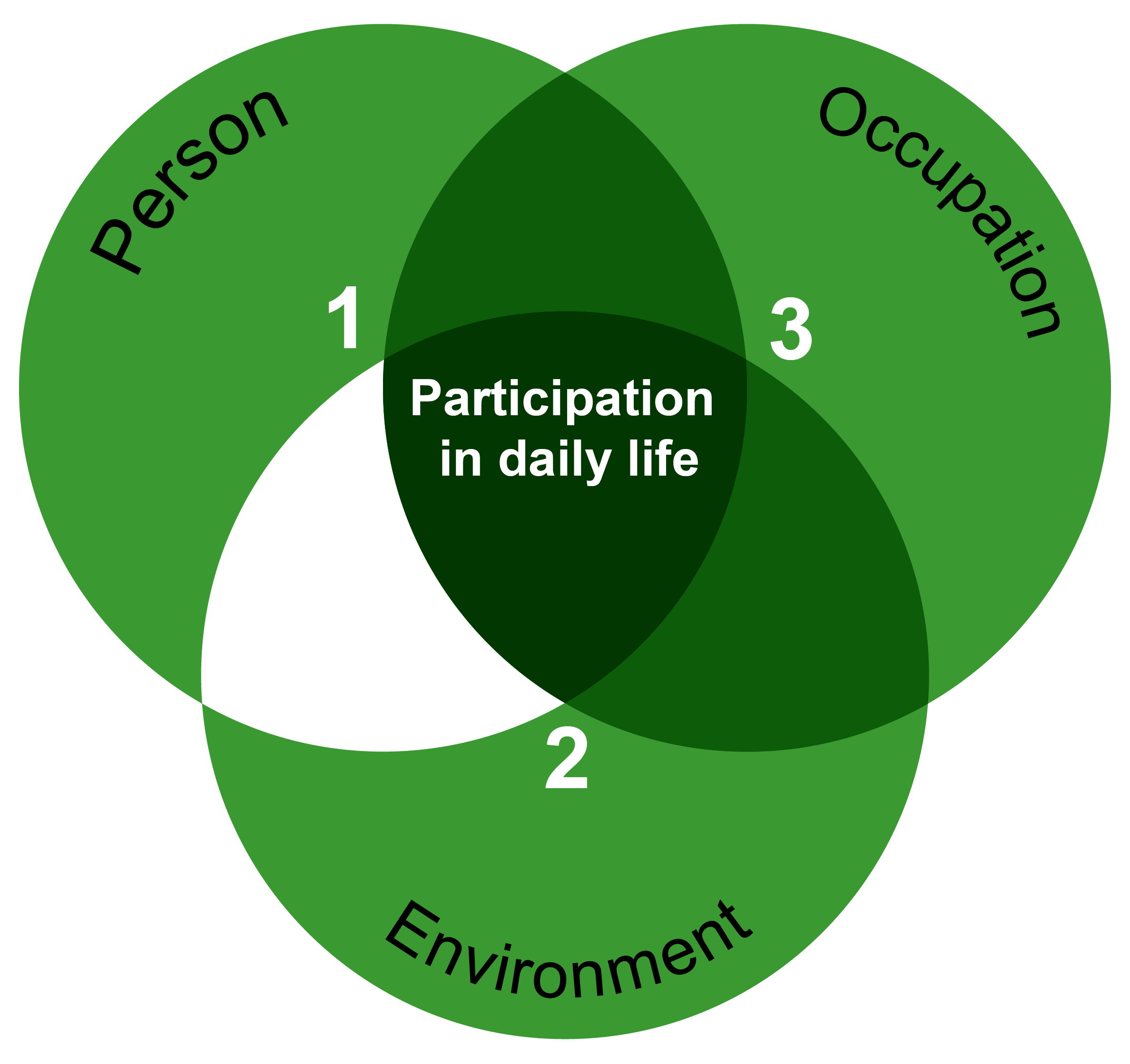
Source: Law et al (1996)
Occupational therapists are most visible to people in settings where people have already experienced a change in their health for example in hospital, in adult social care, in housing, or working with people who have a long-term illness or condition, including physical and learning disabilities and mental health conditions. The adjustments (interventions) an OT enables so that someone can participate in an activity are also visible, for example adaptations to the home.
The OTs professional belief in the impact of occupation on health and wellbeing, and their unique core reasoning skills applied in working with someone are much less visible and valued. As stated in Unique core skills of occupational therapy by Elizabeth Casson Trust.
OTs work with people to understand what matters to them, their hopes and aspirations, their strengths and assets. Using their professional judgement and evidence-based critical reasons to make decisions, they work with people to create a personal plan with goals and adjustments and enable this to be achieved.
OTs have the skills and knowledge to work with people to enable and empower them before barriers to everyday activity escalate, requiring more intervention. Drawing on their unique expertise and experience offers councils, working with their local health and care system partners, an opportunity to realise their ambitions for health and care closer to home, preventing ill-health and reducing health inequalities.
The difference occupational therapists in councils can make
The following sections describe three agendas councils are concerned with, where the principal and strategic occupational therapists engaged in this research believe there is scope to do things differently, building what they have been able to achieve, should the right environment exist. Each section briefly describes:
- What OTs in councils ask of Government so that they are optimised
- Why the topic is important to councils
- What OTs in councils offer:
- The policies, guidance and frameworks underpinning their work
- What their offer looks like now, or could look like
The involvement of OTs in how councils deliver services and achieve outcomes is diverse. In some areas, but not all, what is described already exists: case studies/personal stories have been included to demonstrate what’s possible further in this report.
A clear message throughout this work is that the value of occupational therapy, and OTs in councils, is not recognised nationally. It is recommended that:
National recognition of the value of occupational therapists in councils will be a step towards enabling the government’s short- and longer-term aspirations for the population’s health and wellbeing, and prosperity. This could be achieved through:
1. An occupational therapist/AHP adviser in DHSC (adult social care and integration) who can:
- Educate others’ in the value of occupational therapy, promote OT leadership (professional and strategic) and practice in councils, including in meeting statutory duties
- Provide leadership, identify and enable opportunities for value to be optimised, in developing the ten-year health and care plan, national care service, employment support reform and other Government priority areas eg, mental health service transformation
- Communicate with OTs working in the health and care system, and with other Allied Health Professionals, in support of an integrated workforce and ‘care closer to home’
- Increase local authority confidence that the government is serious about prevention in the widest sense, not limited to the NHS
- Promote and advise on investment in research
2. Investment in enabling a better understanding the value of prevention, specifically increasing the evidence of the value of occupational therapy in adult social care and population health.
Preventing, delaying and reducing the need for care and support
This section is in two parts, considering the contribution of occupational therapists to prevention as defined by the Care Act 2014: firstly, the role of OTs working in and alongside adult social care, followed by a section on the role in relation to adapting the home environment.
The OT in councils ask
OTs in councils already contribute to enabling ‘gloriously ordinary lives’, working in adult social care to meet Care Act duties, with NHS colleagues, with people and communities. Making visible this contribution to preventing, delaying and reducing the need for care and support is essential to government plans to ‘rescue, reform and revolutionise’ the NHS. This could be achieved through:
1. Investment in a review of local implementation of the NHS Intermediate Care Framework from an OT working in adult social care and housing perspective, to understand progress, identify positive practice and areas for improvement, and for improvement action to be resourced
2. Nationally led workforce planning and development. This needs to:
- Recognise that adult social care is a specialist subject and that, with the right environment, occupational therapists working here could contribute to developing the NHS workforce (including NHS OTs) in this subject area.
- Recognise local government as an equal partner in workforce modelling for occupational therapists, alongside other registered health care professionals working in adult social care.
3. Enabling local authorities to more effectively understand the need for occupational therapy in adult social care to achieve outcomes that matter to people, and the impact of the person-centred and preventative activity undertaken by OTs in adult social care (also in public health, housing and economic growth terms). Ideally this would be achieved as part of ADASS’s ask to unlock the potential of integrated data across health, housing, welfare and social care.
4. Investment in the evidence base underpinning occupational therapy preventative practice in adult social care, and dissemination, including to acknowledge that more people are living in the community with greater acuity, and that this trajectory is set to continue.
Enabling the things that matters to us: the role in prevention in the Care Act 2014 context
Summary
- The occupational therapy profession’s philosophy aligns with the underpinning principle of the Care Act 2014, that ‘the core purpose of adult care and support is to help people achieve the outcomes that matter to them in their life’, enabling them to live as independently as possible for as long as possible.
- The Act gave occupational therapists in councils more freedom to practise, using the full range of professional reasoning and skills, to prevent, delay and reduce the need for care and support.
- Councils have not been sufficiently or sustainably funded to deliver the Care Act. Instead, financial challenges experienced by local authorities amidst increasing and changing demands for care and support from their local population, have limited the OT contribution to prevention in councils.
- Being able to achieve what was envisaged by the Care Act, and the more recent shared vision for care and support (above), will contribute significantly to the government’s ambition for everyone to live longer, and in the short-term it is essential to enabling an NHS fit for the future.
- OTs in councils already play a role in the services that enable the NHS to meet patients needs, from hospital discharge and reablement, to enabling people to stay safe and well in the community, but there is more they could contribute, and earlier, to benefit more people and reduce pressures.
- Councils want to be more prevention focussed. The LGA’s asks of central government for additional and sustainable funding for councils, and help to embed prevention as an underpinning approach in all its work – including in adult social care, and action to build the evidence base on the effectiveness and contribution of different forms of preventative spending will all enable OTs to play a more effective role, including working with commissioned services to improve quality, efficacy and cost-effectiveness.
Why the OT offer is important
As discussed in the introduction, an ageing population and more complex needs for care and support are placing immense pressure on councils. The cost of provision is rising, and workforce challenges are significant. There are waiting lists for assessments of care packages and home adaptations, and unmet needs impact individuals and communities. Councils and Directors of Adult Social Services (DASS) are advocating for a focus on prevention and sufficient resources to address these challenges.
What OTs in councils offer
The framework for prevention in social care, and occupational therapy
The Care Act 2014 established a framework for prevention in social care, emphasising the promotion of wellbeing and independence. As detailed in the introduction, local authorities are required to provide or arrange services to prevent, delay, or reduce care needs, identify available prevention services, and promote diversity and quality of services. Occupational therapists play a crucial role in this framework, effectively preventing, reducing, or delaying needs for care and support.
Examples of occupational therapy in prevention
Diagram two: Occupational therapy in social care
Source: RCOT 2019
Social care occupational therapists are specialists and making the best use of this expertise is essential for councils to meet their Care Act statutory duties and wider ambitions for their local population.
In this research, principal and strategic occupational therapists described barriers to them optimising their contribution to prevention:
- In adult social care, councils and across the local health and care system, there isn’t a shared understanding of the populations’ needs and what this suggests preventative services should look like. Within this, who needs and would benefit most from OT input? Understandably the trajectory of demand on adult social care and associated pressures means OTs are increasingly working with people with multiple needs which are complex to meet – increasing acuity. Not only does this limit their capacity to contribute to prevention, but their practice in this area is not felt to be underpinned by a robust evidence base, which presents risks professionally, and to councils.
- Information systems designed to capture and report local authority performance in adult social care do not have the capability to capture the OTs contribution beyond number of people waiting for and receiving an assessment. Individuals have sought to create workarounds, but this is a challenge experienced across councils and would benefit from a national and consistent approach which would be a better use of resources, and enable comparisons
- Invisible in the data, occupational therapists aren’t included in conversations where they could add value, missing opportunities for their leadership, knowledge and expertise to contribute. In those councils where there is an occupational therapist in a senior and strategic role, inclusion in strategic decision making is improving, but not all councils have such a role, or the role includes responsibility for services which take priority. Research undertaken in the West Midlands supports the view that where Councils are not positioning occupational therapy prominently, they are missing out on substantial cost savings from preventative interventions and the best possible outcomes for people and budgets.
- There is much scope to reduce demands placed on OTs in social care so that they may shift their focus, for example through:
- OTs in social care increasing the competence and confidence of others’ in frontline services in the NHS, in council ‘front door’ and housing services, and in the community, to act and act earlier. This includes adopting trusted assessor models for care, support and home adaptations.
- The development of integrated, person-centred, workforces across care pathways with NHS and other partners. When introduced the Discharge to Assess model (D2A) ‘home first’ approach intended for most assessments to be undertaken in the community, with staff working in acute hospital settings shifting to community settings. This has not happened everywhere. It can be the case that individuals’ have their needs assessed more than once, for example by an NHS OT or OT assistant, only for this assessment not to be holistic and/or information from this assessment is not shared with the council’s OT (social care and housing). People are passed from one service to another, delays are incurred, and issues arise.
Opportunities for OT expert input to contribute more to prevention include:
- In other council service improvement and design, for example in housing services such as housing options and tenancy support, and hoarding.
- Working with the voluntary and community sector to enable access to communities who may not approach the council, and where there is potentially more scope for an OT to practice, but needs appropriate support.
Kirklees Council: improving referral routes and assessment times
Kirklees Council created a dedicated social care occupational therapy (OT) team in 2020. The team assess people before they are referred to social work teams, improving outcomes earlier and preventing the need for some to be referred to those teams. There are nine OTs and three assistant OTs with freedom to respond to people's needs using rehabilitative, social care and assistive technology interventions. It can directly assess needs, reducing wait times and referrals at every stage. It allows for quicker intervention and helps people live independently for longer, saving the council £1million in 2022-23. This team is now also recognised as demonstrating strength-based practice and it is used as a resource to support other social care colleagues.
Nottingham City: Care Act reviews completed by OTs and return on investment
In Nottingham City, Care Act reviews completed by occupational therapy practitioners saved about £1,166 per year, compared to reviews by social work practitioners that saved an average of £659 per year (West Bridgford Wire, 2024). In Telford and Wrekin over £900,000 worth of commissioned care was avoided by an occupational therapy project. There were positive examples of occupational therapy practice, regardless of the size of the service, in every single local authority that contributed to this report.
The place we call home: enabling healthy, safe and suitable environments
This section is specific to people for whom an adaptation to the home, or assistive technology, would overcome barriers to participation; they already have a need. The role of OTs in relation to home as a wider determinant of health and from a population health perspective is discussed in ‘improving and protecting the public’s health’.
Summary
- The right home environment is essential to our health and wellbeing, and it is the setting within which we participate in most everyday activities. The home can present barriers to participation, for disabled people, as we age, for people who experience a change in their health, for those with caring responsibilities
- Ambitions to enable people to live healthier lives in the community, as independently as possible, preventing, delaying and reducing the need for health care, care and support will only be possible if barriers to participation in activities in the home are addressed
- When delivered in a timely manner, equipment, adaptations and assistive technology play a crucial role in preventing, delaying or reducing the needs of adults either for care and support or the needs of carers for support ie, provision could be considered as enabling local authorities to meet their general duty under the Care Act 2014.
- The inclusion of the Disabled Facilities Grant (capital grant contributing to the cost of home adaptations) in the Better Care Fund in 2015 was in recognition of the importance of ensuring adaptations are part of an integrated approach to housing, health and social care locally, and to help promote joined up local person-centred approaches to supporting communities.
- In councils, there is a collaborative approach to provision. Occupational therapists, working alongside housing, allied health and other health care professionals, play an important part in enabling the right equipment, adaptations and assistive technology, particularly in assessing and advising on what is necessary and appropriate
- In their leadership and strategic role, OTs can also enable:
- Improvements in timely access to equipment, adaptations and assistive technology, working across health, care and housing systems, preventing the escalation of care and support needs
- A more proportionate use of skills in the workforce; taking a person-centred approach, and developing others in the workforce to be confident in understanding what’s needed to overcome barriers in the home
Why the OT offer is important
The timely provision of equipment, adaptations and assistive technology (adaptations from hereon), and information about these, play a crucial role in preventing, delaying and reducing health, care and support needs. They enable:
- People with no or low-level needs, and those around them, to make informed decisions, have choice and control, so that they may act in a timely way before a health crisis, or care and support needs develop. This could include signposting to a retailer and/or support to install a grab rail, which may prevent a fall, enable someone access to their own home or to reduce reliance on other family members / carers
- Disabled people, people with a long-term condition and people as they age to live independently and safely for as long as they choose eg, addressing issues in the home that present a risk to someone with dementia, or which may contribute to behaviours of concern – delaying and reducing the need for care and support in the home, or elsewhere
- People who have experienced a change in their health and/or mobility to regain skills and confidence to participate in activities at home and in the wider community (reablement and rehabilitation).
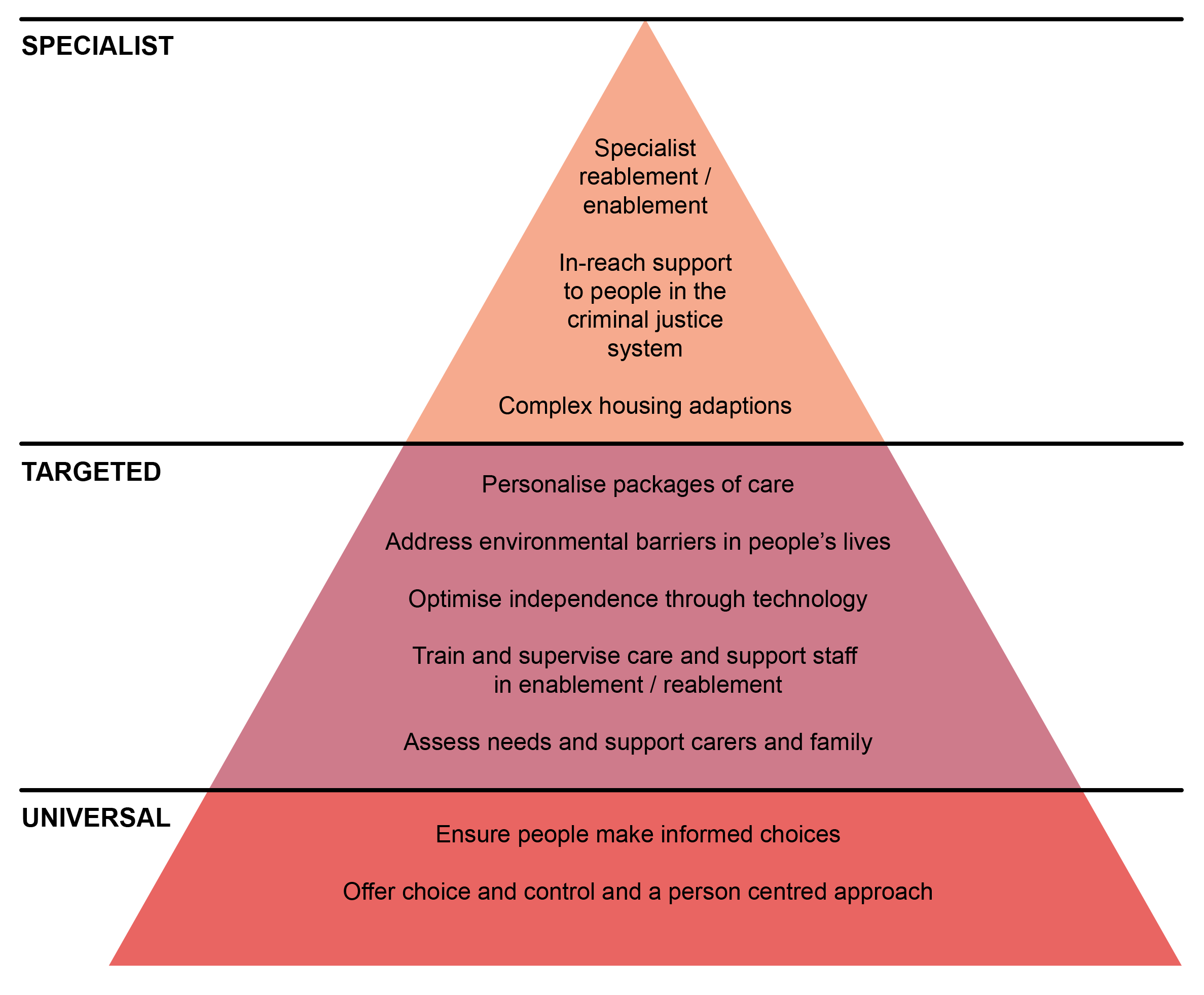
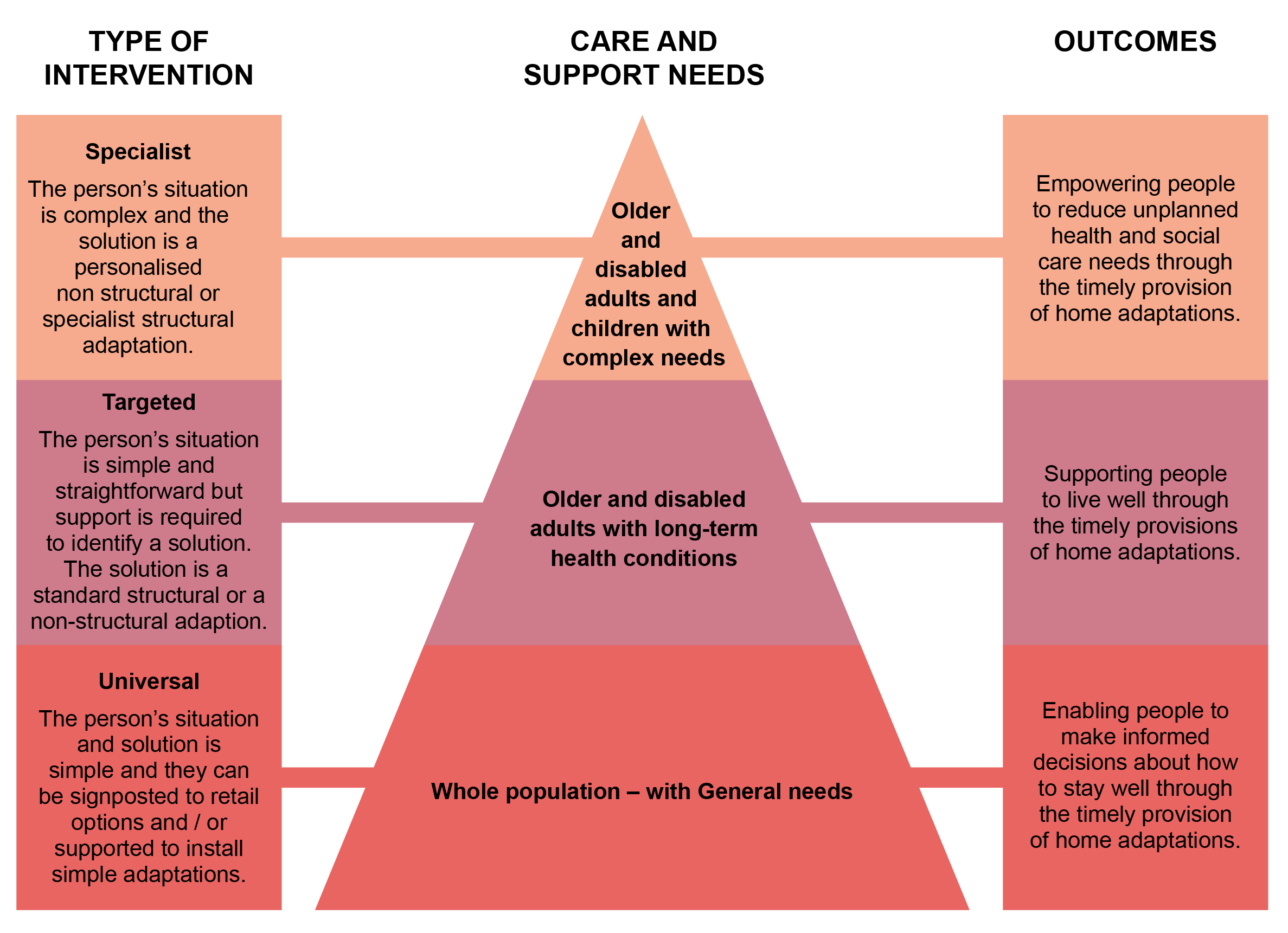
Universal, targeted and specialist interventions
What OTs in councils offer
The framework
The Care Act 2014 and the Housing Grants Construction and Regeneration Act 1996 provide the legislative framework for the provision of adaptations, with the former suggesting adaptations in reablement and rehabilitation is an example of a preventive service.
Care Act Statutory Guidance requires that assessments of need should be undertaken by skilled, knowledgeable, competent and appropriately trained people, and suggests that registered occupational therapists and social workers have such expertise. However, there is flexibility in how this expertise is used locally and compliance suggests their involvement in more complex assessments, and that they have a role in supporting staff in first contact with people, who must have the benefit of appropriate training and access to professional support.
Care Act 2014 wellbeing principles and adaptations
Synergies between Care Act and the DFG
| Care Act | DFG |
|---|---|
| Managing nutrition | Access to facility to prepare meals |
| Maintaining personal hygiene | Access to bathing facilities |
| Managing toilet needs | Access to toilet facilities |
| Being appropriately clothed | |
| Able to be safe within home | Make dwelling safe |
| Ensuring a habitable environment | Improving or providing heating if needed by the disabled people |
| Developing or maintaining relationships | Access to a principal family room |
| Accessing work, education, training | Facilitating access to and from garden |
| Making use of community facilities or services, including public transport | Access to an from dwelling |
Source: Anita Mottram
In addition to local authority responsibilities, for people who need ongoing care and support from health and care professionals because of disability, accident or illness, and are eligible for NHS Continuing Health Care funding, the Integrated Care Board and NHS providers are responsible for adaptations.
The policy and funding framework for adaptations is not straightforward. Inclusion of the mandatory Disabled Facilities Grant (DFG) for major adaptations in the Better Care Fund in 2015, and 2022 government guidance for local authorities on the delivery of the DFG have attempted to enable better outcomes through joint working within councils and in the local care system. It remains the case that the operating environment within which OTs working in council and NHS settings may not enable the most effective use of their expertise, in turn impacting on ease of access and delivery of timely adaptations.
The 2023 NHS Intermediate Care Framework, recommending that people should have access to community-based, therapy-led reablement and rehabilitation interventions once they’re discharged from acute (physical) inpatient settings and virtual wards on intermediate care pathways, suggests that integrated care systems will want to improve how they use their workforce to enable this. This is an opportunity to consider how ease of access to adaptations can be improved, making the best use of occupational therapy expertise across health, care and housing systems.
In recent years there has been much work by national bodies such as Foundations and RCOT. to improve access to timely equipment and adaptations. The Adaptations Without Delay framework provides the basis for:
- Enabling a proportionate response ie, getting the right response at the first point of contact, followed by signposting people to the right type of service (universal, targeted, specialist) – in turn reducing delays and the likelihood of people waiting on lists for assessments they do not require, and potentially for their health, care and support needs to escalate consequently.
- Supporting the development of a workforce with appropriate knowledge and skills, placing people at the centre of a process that ensures they receive the right level of assessment from a workforce that has the right level of skill and knowledge to assess and recommend adaptations.
Improving and protecting the public’s health
The OT in councils ask
The contribution all OTs could make to improving and protecting the public’s health has been increasingly recognised, nationally through a UK Allied Health Professionals public health strategic framework, and locally through joint work with public health teams on system approaches to prevention and action on health inequalities. There is however much scope for the role of OTs in councils to be optimised, benefitting many more people locally, and for this to enable councils to recruit and retain more OTs as there are more opportunities for impact and career development.
This could be achieved through:
- National policy, and support to AHPs, explicitly recognising the role of OTs in councils in improving and protecting the public’s health and enabling this locally, for example through specific support and guidance, learning and development opportunities for councils, OTs, public health professionals, elected members and other system partners
- Investment in research to better understand the value and potential of OTs in councils in improving and protecting the public’s health and reducing health inequalities, with particular focus on:
- the system leadership role of principal and strategic occupational therapists
- populations not in need of adult social care, across the life course
- populations experiencing the most significant health inequalities and likely furthest from accessing health and care services eg, people in contact with the criminal justice system, those experiencing homelessness etc,
- optimising what OTs understand about their local populations that could be applied ‘upstream’ to prevent and protect health.
In relation to ‘home’ as a wider determinant of the population’s health, this could be achieved through:
- The Government requiring new development and regeneration plans and projects to engage with OTs who have the knowledge and expertise to advise on inclusive design – this would need additional funding.
- Investment in new opportunities for OTs, and others working in new housing development and regeneration, to acquire knowledge and competency in inclusive design.
Summary
- Occupational therapists in councils contribute in many ways to protecting and improving the public’s health, but this isn’t widely understood
- The role of Allied Health Professionals in public health is gaining momentum in the UK: a national strategic framework aims to promote and support roles; the Health and Care Professions Council requires occupational therapy and other registrants to demonstrate proficiency in promoting public health and preventing ill-health.
- As an outcomes-focussed clinical profession, OTs in councils are ideally placed to contribute strategically, and in practice, to local health and care system redesigns and integration beyond the NHS and social care
- They bring a person-centred approach to enabling people to stay healthy at home, in the community; their model is social, not medical
- They are knowledgeable in NHS pathways of care, including from hospital to home, and will likely have a relationship with, and understanding of, workforces in these pathways
- Their experience can contribute to improvements in tackling inequalities in health care: access to, experience of and outcomes
- With their expertise and knowledge in prevention, the wider determinants, and health inequalities – across the life course - there are opportunities to realise the occupational therapy potential, with examples including:
- Supporting the adult social care workforce to realise their public health contribution
- OT leadership in reviewing and redesigning the local prevention offer to benefit the wider population, in addition to people who have care and support needs and their carers
- Enabling a population health approach to accessible and inclusive homes
- Targeting OT expertise to benefit populations experiencing health inequalities, for example to survivors of domestic abuse living in refuge accommodation
- Using their skills in motivational interviewing, behaviour change techniques, trauma informed practice, amongst others, to enable individuals to take action to improve their health and wellbeing
- Supporting people to remain in, return to, or obtain work including through training others’ in the workforce.
Why the OT offer is important
Local councils and the LGA believe a new focus on prevention and wider services for the community is needed. It’s essential to deliver the best outcomes for people, and to avoid spending more later when people’s needs escalate; increasingly younger – working-age- people are experiencing ill-health. Lord Darzi’s independent review of the NHS concurs.
Preventive services need to form part of overall service design for local communities, adopting person-centred approaches across the age range. In addition to investment in adult social care, a comprehensive approach includes (not exhaustive):
- Targeted support, including for children and young people at risk, with effective, sustainable support for children and young people with SEND [OTs provide support to this population: this has not been covered in this report)
- Public health interventions, which are well-evidenced to prevent ill-health, support a healthy, productive workforce, and significantly reduce future health and social care costs
- Prevention in housing, homelessness and supported housing services, to avoid serious health impacts
- Support for financial hardship and debt, enabling people to meet their essential living costs and alleviating the stress and social exclusion that accompany poverty.
- Culture and sports activities, which promote good physical and mental health, community cohesion and resilience, and support a healthy workforce.
To make sustained progress in improving population health outcomes, the Association of Directors of Public Health (ADPH) suggests there needs to be a whole system approach and concerted action to address the wider determinants of health. In addition to a shift in the health and care system towards prevention of ill-health and tackling health inequality, ADPH calls for extension of integration of services beyond the NHS and social care to the wider range of services engaging with the population, taking a place-based approach and working collaboratively to ensure people lead healthy and fulfilling lives. Key enablers of the public health system are: a fit for purpose workforce, funding aligned with population need, a strong evidence base and good quality data.
What OTs in councils offer
The framework for the OT offer to public health
In addition to providing person-centred support for people who need health and care services, Allied Health Professionals (AHP) – of whom occupational therapists are one – have long been acknowledged as part of the wider public health workforce: improving and protecting the public’s health, in leadership roles and in their work with individuals, across the life course.
AHPs Deliver (2022-27), the national strategy for AHPs in England, acknowledged that AHP skills ‘are often underutilised in enhancing the public health and prevention agendas. AHPs’ contribution to the reduction of health inequalities should be considered in the redesign of patient care pathways.’
Key approaches underpinning the AHP contribution to public health include:
- taking a population approach
- using data and evidence to inform decisions
- focusing on prevention
- considering the wider, societal determinants of health and wellbeing, and focusing on reducing inequalities.
The UK’s AHP Public Health Strategic Framework 2025-2030 has a vision that public health is a core part of all AHP roles and that the positive impact on public health by AHPs is recognised and valued. It’s five goals are:
1. To develop the AHP workforce to improve and protect the health and wellbeing of individuals, communities and populations, and to embed public health and prevention within the culture of organisations and services where they work
2. For AHPs to ensure individuals and communities have equitable access to health and care services, co-producing services with people and working collaboratively to empower choice and control
3. AHPs will deliver services and interventions that are economically and environmentally sustainable
4. AHPs will be able to demonstrate their contribution to improved outcomes from individual to population level through delivering evidence-based practice, using data and intelligence to guide decision making, design new models of care and show impact
5. AHPs will be empowered to lead and influence across the entirety of the health and care landscape to improve health outcomes for individuals, communities and populations
The RSPH handbook of profession-specific descriptors for public health reinforces the AHP’s role in public health, providing examples of how occupational therapists contribute to the four domains.
Examples of the OT contribution to the four domains of public health (Source: RSPH 2024)
Health protection:
- Occupational therapy leadership within the fire service to reduce fire risk and address health and wellbeing in vulnerable communities.
Wider determinants:
- Addressing occupational deprivation as a way to reduce health inequalities.
- Occupational therapy has a sustainability action plan to promote greener practice and contribute to wider health.
- Occupational therapy report on health equity.
- Occupational therapy - social prescribing active signposting.
- Occupational therapy children - social prescribing active signposting.
Population healthcare:
- Occupational therapists work with condition specific charities to provide treatment and support for people and their carers.
- Provision of therapeutic boxing for psychiatric intensive care unit.
- unlocking the potential of children and young people.
Health improvement:
- Occupational therapy and social prescribing
- housing adaptions report
- Sport for confidence and stay connected: creating an online physical activity service.
- Occupational therapy community 360 social prescribing
- Occupational therapy - AHP prescriber social prescribing.
Health inequalities
The role of AHPs in reducing health inequalities (systemic, avoidable and unfair differences between populations, within populations or across a socio-economic gradient) has also received attention, with Public Health England and NHS England commissioning the King’s Fund to research and develop a framework in collaboration with all AHP bodies, including the Royal College of Occupational Therapists. The framework supports professionals to consider their role through six lenses:
- as an individual,
- in their role in caring for individuals,
- being a part of a team and service,
- their involvement with communities and networks,
- their involvement in the wider health and care system,
- and their efforts to nurture the future.
The Fund notes that OTs have taken part in their leadership for population health programme, and in doing so, increased understanding amongst other system leaders about the role AHPs play in tackling health inequality, and population health more widely.
My role in tackling health inequalities: A framework for allied health professionals

Occupational therapists are registered with the Health and Care Professions Council; from September 2023 a new ‘promoting public health and preventing ill health’ proficiency standard was introduced for all registered professionals, recognising they’re part of a larger health system and play an important role in promoting good health. In practice occupational therapists already meet the standards described, for example understanding their role in preventing ill-health, empowering and enabling individuals to play a part in managing their own health, and understanding how social, economic and environmental factors (wider determinants of health) can influence a person’s health and well-being.
Finally, the Principal and Strategic Occupational Therapists Network contributed their knowledge and expertise from working in councils to the most recent addition to the All Our Health Programme resources, Adult Social Care public health tips, to support the social care workforce to increase their knowledge and action on public health approaches.
All our health: adult social care public health tips
Tip 1: What public health is and how it links to what you do.
Tip 2: Address the factors that impact people's health.
Tip 3: Tackling health inequalities.
Tip 4: Support health promotion.
Tip 5: Embed prevention.
Tip 6: Support for mental health.
Tip 7: Infection prevention and control is public health.
Tip 8: Care for ourselves.
Tip 9: Help people age well and maintain independence.
Tip 10: Address the effects of climate change.
Source: Gov.uk 2024
Healthy homes as a wider determinant
The role of OTs in relation to people for whom an adaptation to the home would overcome barriers to participation is discussed in the earlier section, in relation prevention and people who already have a need.
The government has an ambition to build 1.5 million new homes in the next five years, presenting an opportunity to think differently from the start about a household’s changing needs over time, and designing homes to be inclusive of these.
A healthy home must be suitable for all those living there, enabling them to continue to participate in everyday activities that matter to them. For disabled people, and people as they get older – growing populations - this is particularly important, but there are wider population benefits from accessible and inclusively designed homes.
There is also an economic argument for inclusive design in new homes; at the outset there may be no, or minimal additional cost, and can negate the need for subsequent costly adaptations at a later stage, and associated health, care and support need costs.
Recent research commissioned from the London School of Economics from Habinteg makes the case for accessible homes to improve health and wellbeing and enable participation in society, across the life course, reporting that:
- 400,000 wheelchair users in England live in unsuitable accommodation
- 20,000 are estimated to be on local authority waiting lists for a wheelchair user home, waiting on average 47 years to be offered a suitable new-build property
- Positive financial values calculated, combining reduced public expenditure (for example to the NHS and local authorities), with revenue generation eg, through people being able to participate in paid work are:
- For a working age wheelchair user, the benefit of living in a wheelchair user home can be valued at £94,000 over a 10 year period
- For a later years wheelchair user household (aged 65 and over), the benefit could be £101,000 over a 10 year period
- For a household with a child who is a wheelchair user, the benefit of living in a suitable wheelchair user home could be £67,000 over a 10 year period
ADASS 2023 Autumn Survey found that over 90 per cent of Directors of adult social services agreed that more accessible and adaptable homes, extra care accommodation, supported housing and Shared Lives Housing would improve outcomes for people drawing on care and support. Over 70 per cent said that increased national investment in these specialised housing options would save them money on adult social care which they could reinvest in better meeting more people’s needs.
Recognising the importance of suitable homes for older and disabled people the government consulted on options to improve accessibility of new homes in 2020, and subsequently announced that it intended to mandate the accessible and adaptable standard of the Building Regulations. These set out minimum expectations; there is more scope to improve accessibility, and outcomes for people and communities.
To address common misunderstandings and missing detail in the Building Regulations and inspire design that goes beyond improving physical access to consider aspects such as visual and sensory access, Habinteg Housing Association and the Centre for Accessible Environments have recently launched an Inclusive Housing Design Guide, authored and peer reviewed by specialist housing occupational therapists and inclusive environment specialists.
What OTs in councils offer
Occupational therapy leadership, capacity and capability varies between councils: the current contribution to public health will relate to this.
The current contribution to the public health agenda is primarily through the role of occupational therapy in adult social care, particularly in preventing ill-health (population health care) (see previous section):
- For many people, their contact with an occupational therapist in councils relates to a health condition, including following hospital treatment. The OTs role in this space can be considered population health care; OTs engaged in this research feel this is where their main contribution to public health currently is, but during these contacts, they also address issues in other domains, for example health improvement through conversations about behaviours
- OTs already work in ‘front-door’ service offers to people who have no ongoing care or support need, including in the working-age population
There is a growing number of occupational therapists with specialist expertise in design of new build homes, or refurbishment. Involving occupational therapists in new build, regeneration and refurbishment projects can be the most effective way of achieving accessible design and adaptability to meet the populations’ changing needs in the long term, advising on how to prioritise and incorporate the best aspects of accessible design guidelines into new build and refurbishments. They can also work with residents to develop design evaluation tools that can inform future schemes.
Principal and strategic occupational therapists believe they could add further value through working with their local public health team to:
- Provide leadership and/or contribute strategically to local authority, health and care system work intended to improve health and wellbeing outcomes and reduce health inequalities, including reviews and redesigns intended to shift health care into the community
- Develop their understanding of public health priorities and services locally, and exploring options to optimise their contribution, with support from the public health team and partners
- Educate public health colleagues in the role of occupational therapy, and their role in the council, particularly in terms of prevention
- Identify opportunities to:
- Share knowledge, expertise and resources, for example public health expertise in research to better understand the value of OT locally, and OT expertise in understanding the health and care system from the user perspective
- Take a population health approach to addressing wider determinant of health issues eg, the need for accessible and inclusive homes, and how this will be met through new homes and the provision of technology, equipment and adaptations (collaboration with the local housing authority is essential: legal duties lie here), and others’ eg, the Fire and Rescue Service
- Make better use of ALL local prevention resources, to meet the wider population’s needs, for example a universal information, advice and support offer, drawing on existing OT knowledge of the local population and experiences of meeting needs
- Better understand and develop the OT contribution to improvements in health and wellbeing outcomes for the ‘working age’ population (‘ownership’ of this life course may sit with the local public health teams)
Inclusive growth: Everyone is better off
For everyone to be better off, we need an employment, and skills offer shaped by local areas and inclusive of people whose health, or of those they care for, presents a barrier to participation in work and learning.
The OT in councils ask
The occupational therapy profession was founded upon principles related to the benefits of work and supporting people with health conditions to gain or return to paid employment. This hasn’t been recognised in recent policy, and practice opportunities have been limited. With the publication of the Get Britain Working White Paper, the Government intend to better integrate health and the skills system, so there is an opportunity to integrate the role of OT into the skills system, which can be achieved through:
- Enabling OT participation in the Government’s plans, with councils, to reform employment support and deliver the Connect to Work programme.
- New research to explore the full potential of the OT role in enabling improved work and learning outcomes, and propose what workforce, training and education would be needed to achieve this.
- An increase in opportunities for OTs to attain or refresh competencies in vocational support.
- Government action to address the barrier to work and learning presented by the means tested Disabled Facilities Grant for home adaptations; access to the working-age population is restricted.
Summary
- Work (defined as the application over time of effort, skills and knowledge put into either paid or unpaid activities) is an essential occupation to ensure good health and wellbeing. Supporting people to remain in, return to, or obtain work is a key function of occupational therapy.
- Occupational therapy in councils has significant potential to contribute to local ambitions for inclusive growth and productivity.
- OT leadership, and participation, in designing and delivering an effective local skills and employment offers will likely increase their impact:
- Enabling people to access advice and support earlier about work and learning, for example at the ‘front-door’ of the council, and in the community from trusted organisations.
- Supporting people to retain or regain their skills and confidence so they may live independently following illness or other life-event (vocational rehabilitation).
- Increasing capacity and capability in the social care, health and wider workforce eg, housing, to ask about work.
- Occupational therapist input will be particularly beneficial to enabling people who face multiple barriers to their participation in work to overcome these, including ill-health and long-term conditions, caring responsibilities, the home environment and access to work.
- OTs in councils have local knowledge of barriers to work, and of the community-based organisations who offer opportunities to gain and develop skills eg, through voluntary work.
- Every area will be running the Connect to Work programme starting from 2025/26, with some Mayoral Combined Authorities running trailblazing programmes to try new approaches to tackling economic inactivity through health, growth and skills. Accountable bodies will be encouraged to engage with support organisations to generate participants in the Connect to Work Programme.
Why the OT offer is important
The LGA’s ‘work, health and growth’ guide, developed in partnership with the Office for Health Improvement and Disparities, provides local councils with a strong business case to improve work and health and economic growth outcomes in their local area.
The evidence underpinning this is:
- Work is good for people’s health and, that when people are in good health, they are more likely to find, remain in and be productive at work.
- Unemployment and economic inactivity through long-term sickness are associated with worsening health outcomes with a negative impact on individuals, communities, and wider society.
- Once economically inactive through ill health, the data shows that few people move back into employment.
- Managing ill health at work and supporting people who experience ill health to get back into work is critical for improving population health outcomes, tackling health disparities and realising the wider economic benefits that come from increasing participation in the labour market.
While unemployment is currently relatively low, the number of people who are economically inactive (people aged 16–64 who are not in employment, who have not sought work in the last four weeks and /or who are unable to start work in the next two weeks) in the UK continues to rise, estimated to be around 9.3 million in the period May-July 2024. This includes people whose long-term ill-health is the primary reason for inactivity, estimated to be 2.83 million people in the UK in February to April 2024.
Health Foundation analysis also draws attention to the 3.7 million working-age people who are in work with a health condition that is ‘work-limiting’, that this number has increased over the past decade and that this trajectory is likely to continue. The Office for Budget Responsibility estimates that the rise in working-age economic inactivity and worsening health has already added £15.7 billion to annual borrowing since the pandemic.
In setting out its Missions, the Government acknowledged that too many people are out of work or not earning enough and that long waits for treatment of health conditions, particularly mental health, are contributing to the rise in economic inactivity. Also, that one in eight young people are not in education, employment, or training, with those lacking good qualifications and with poor mental health facing particular disadvantages.
Within councils in England, the number of employees on long-term sick leave was estimated to be around 10,000 people in February 2024, with 58 per cent of councils reporting a rise compared to 2019.
A multitude of national employment and skills related schemes and services has resulted in disconnected and ineffective employment support for service users and employers which fails to adequately reflect differences across regions.
Lord Darzi’s independent review of the NHS noted that ‘while public debate on social care tends to focus on the needs of older people, there are very significant needs for many children and working age adults with disabilities’.
The ambition
To achieve inclusive growth, local government has a crucial role to play. We welcome the ambitions set out in the Get Britain Working Paper and Connect to Work Programme, which is a step in the right direction towards a devolved and integrated local service.
The Get Britain Working White Paper will promote higher employment and reduced economic inactivity, helping individuals enhance their skills and transition to better jobs. The White Paper has three strategic pillars:
- A modern Industrial Strategy and Local Growth Plans to generate quality jobs nationwide.
- Improving job quality and security through the Plan to Make Work Pay.
- Major reforms to employment support by integrating skills and health.
Every area will have a Local Get Britain Working Plan (LGBWP) to tackle economic inactivity. These plans will be developed by mayoral authorities where they exist, and across groups of local authorities elsewhere. LGBWPs will be backed up by a new supported employment programme, Connect to Work, grant funded to all of local government, starting with £115 million going to local areas in 2025/26 as the first strand of these plans. Some mayoral authorities will go further by trialling new ways to join up work, health and skills.
The White Paper broadly reflects the LGA’s ambitions for an integrated employment and skills offer (Work Local model), linked to local services and meeting local need, and requiring councils, businesses, local further education colleges and other local bodies to work together to deliver within a supportive national framework. A devolved employment and skills service, the Work Local model would have three interlinked offers:
- Youth Pathways to help young people (16 to 24) ‘not in employment, education or training’, or at risk of NEET, find their first job or put them on a career path.
- Working Futures for adults who are disadvantaged in the labour market, and who need personal support to find work or better work.
- Skills for All to provide a better match of skills supply and demand, a skills and learning offer linked to local careers advice and jobs, and promote lifelong learning.
The Health Foundation also advocates for better ways to support the workforce, including:
- Supporting people to remain healthy in the first place and providing rapid support when health starts to deteriorate and affect employment.
- Increasing flows back into work with tailored support to improve health and tackle barriers to work.
- Delivering interventions for groups particularly at risk of being out of work with ill health, such as people with low qualifications, those under the age of 25 years and people aged 50 years and older.
- Taking a tailored approach that accounts for local differences in health and other barriers to work, ensuring local services can work together effectively.
What OTs in councils offer
Work is integral to the ethos of the occupational therapy profession: it was founded upon principles related to the benefits of work and supporting people with health conditions to gain or return to paid employment.
Occupational therapists support people and employment services to understand the relationship between a person’s health and the work activities that they carry out in the work environment. Through specific vocational assessments and interventions, they can facilitate change.
Participation in good work: The role of occupational therapy
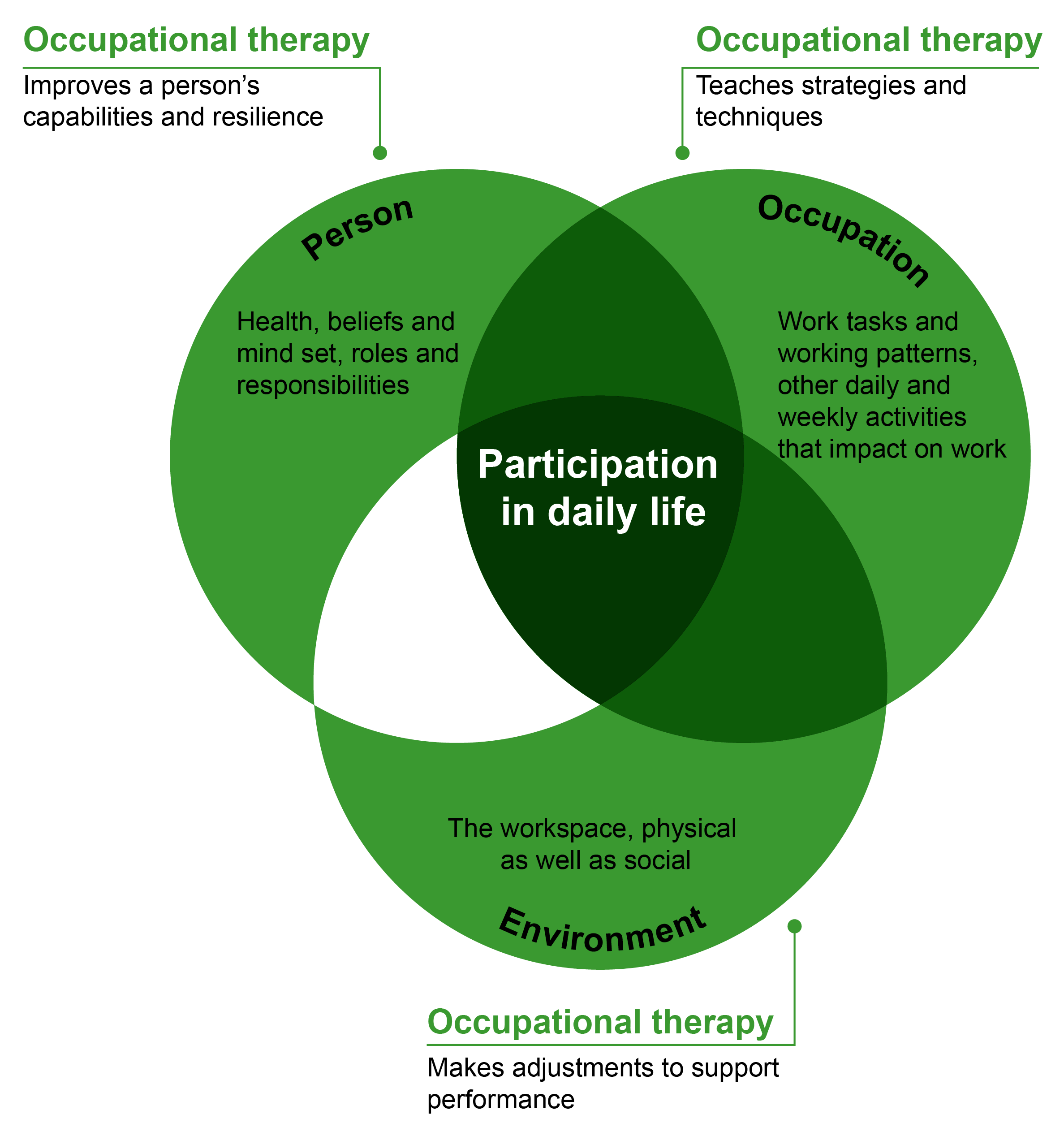
Occupational therapy leadership, capacity and capability varies between councils: the current contribution to ‘everyone is better off’ will relate to this. Working with adults, may currently contribute to this agenda through their role in:
- Supporting and enabling advice and support to people who do not yet have eligible care and support needs, for example in a council’s ‘front-door’ services, or in more targeted wellbeing or population-focussed service offers eg, for people with a learning disability or mental health conditions.
- Delivering support to young people as they transition to adulthood, bridging the gap between home and education (if they’re in this) and independence.
- Assessing peoples care and support needs under the Care Act 2014: participation in education, training and employment is a wellbeing consideration for service users and carers.
- Enabling access to technology, equipment, aids and adaptations to enable people to stay in their home and community, in a safe and suitable home: the home environment can present barriers to work and learning for the individual, their household and carers, and their wider support network.
- Training others’ in the frontline workforce to have conversations about the work and its benefits in their contact with people in the community, including signposting and referring to additional support if needed.
- Managing their own teams, ensuring their health and wellbeing and supporting them should barriers to work present themselves.
- Commissioning existing local universal and targeted offers of support, including from the voluntary and community sector to reach people who won’t engage with the council, where barriers to work and learning may be identified.
- Council workplace initiatives designed to promote and support staff wellbeing.
Populations who Principal OTs and strategic leads feel would particularly benefit from more targeted occupational therapy input, if resources allowed, include (not limited to):
- Young people, as they transition to adulthood, and from education to independence.
- People whose mental health and/or autism and/or learning disability affects participation.
- People who have experience of the criminal justice system.
- People in later life: as they transition from employment to retirement, particularly if this health-related; to live well on their own.
‘Touch point’ opportunities cited where occupational therapy expertise could add more value (not exhaustive) include:
- Autism and learning disability assessments and support services.
- Mental health ‘pathways’, including in community services for people with lower-level needs for support with their mental health.
- For people managing chronic pain and/or fatigue.
- ‘Team around me’ offers to people who experience multiple barriers to participation, which services typically find complex to address.
- For people in or leaving criminal justice settings, including rehabilitation and other community-based services.
- Accessing the Personal Independence Payment (PIP) if extra help is needed because of an illness, disability or mental health condition.
- Keeping people active and engaged in activities important to them outside of care, and work eg, shopping, going to the pub.
Occupational therapists in councils: the workforce
The contribution occupational therapists in councils already, and could, make to improving the health and wellbeing of the local population is relative to the available workforce, and the environment employers can offer: one within which OTs can practice safely and effectively, and feel valued. This section describes what’s known about the OT workforce, the challenges they experience, and asks of the Government to address issues.
Summary
- Occupational therapists are a clinical profession registered by the Health and Care Professions Council; they are autonomous practitioners. There are reported to be 3,200 OTs employed by councils working in social care. An unquantified, but low, number are employed by the NHS but deliver local authority statutory duties under a section 75 arrangement.
- There are over 21,000 OTs employed in the NHS. OTs are also a member of the third largest group of clinical professions in the NHS, the Allied Health Professions.
- In the health and care economy, there are insufficient occupational therapists available to the population; they are on the Shortage Occupation List.
- Councils experience several challenges in recruiting and retaining OTs, essential to fulfil Care Act 2014 and housing duties, including competition with the NHS for the workforce.
- Nationally, workforce modelling and planning for AHPs – including OTs – is led by NHS England; this does not consider the workforce or training requirements of councils and adult social care.
- It is evident that NHSE’s Chief AHP the Deputy AHP in the Office for Health Improvement and Disparity, are supportive of OTs in councils, and integration. However, Government action is needed to ensure that these professionals are being developed, supported and recognised in leadership roles, at the same pace as other AHPs.
- A Chief OT adviser role in Government akin to the Chief Social Worker would give greater confidence that the value of OTs in social care and integration will be optimised; in the short-term seconding an experienced OT already in a leadership position into DHSC could be an effective approach.
- Asks of Government from the cross-sector adult social care workforce strategy are also essential: to attract more OTs; to invest in the development of OTs for example through a national career and skills framework for ASC occupational therapy; to continue investment in the leadership programme for principal OTs to ensure there is a strong talent pipeline for director of adult social services roles.
The occupational therapy workforce
Occupational therapists are on the Shortage Occupation List (SOL): an official list of roles for which the domestic labour market cannot meet the demand to fill vacant posts which can make it easier for employers to recruit internationally trained workers.
Available data about the workforce is limited and considered insufficient to enable local health and care systems and employers to plan for, and meet, their populations’ needs effectively. As mentioned in the introduction, the Royal College of Occupational Therapists (RCOT) continues to seek improvements in workforce intelligence through its new Workforce Strategy. Most OTs are employed in the NHS, but a significant number work independently, contributing to the disparity between registered OTs and those employed by councils or the NHS.
The OT workforce experience
The LGA annual employer standards survey and health check
The LGA’s employer standards for occupational therapists set out the shared core expectations of employers which enable occupational therapists in all employment setting to work effectively and safely. The LGA’s 2024 Employer Standards Survey was responded to by 1,902 occupational therapists. Key findings are:
- A decrease in satisfaction in five out of the eight standards.
- A positive response to questions on engagement with my job and organisation.
- A 12 per cent drop in score for standard 3 (safe workloads and case allocation), driven by new questions on caseload weighting tools and workload allocation policies.
- A significant difference in level of satisfaction between occupational therapists who had experienced a mental health condition in the last 12 months and those who had not.
- Effective workforce planning systems has dropped to the lowest scoring standard.
There were differences in responses across different employers (local authority, NHS Trust (integrated roles), and others). Those employed by local authorities gave an average mean score of 77 per cent, compared to an average mean score of 85 per cent from those employed by NHS trusts.
The Employer Standards survey, also known as the ‘health check’, gives a voice to registered social workers, occupational therapists, and non-registered social care professionals. The key purpose of the survey is to better understand a number of critical questions about the experiences of the social care workforce in England. Funding the Health check is essential to listen to the workforce and create an environment where OTs can thrive. This work supports continuous professional development, improves workforce conditions, and ensures that occupational therapists can practice effectively and safely across councils and Trusts.
RCOT workforce survey 22/23
A survey of the occupational therapy workforce (working in all parts of the health and care system) by RCOT in 2022-23 received over 2,600 OTs responded. Key findings include:
- 86 per cent reported an increased demand for OT services within the previous 12 months. Reasons were varied but lack of capacity in the health and care system, increasing complexity of people’s needs due to delayed interventions resulting in an increased need for OT input, increases in mental health needs and lack of availability of carers were factors many suggested.
- 78 per cent said that their team wasn’t large enough to meet the demand, with longstanding issues of recruitment impacting their ability to provide OT support to meet needs. For some, staff shortages were resulting in long waiting lists. 63 per cent felt they were too busy to provide the level of care they’d like.
- 68 per cent of respondents said that they were under too much pressure at work. 59 per cent rated their work-related stress as 7 or above on a scale of 1 to 10, with 10 being the highest level of stress.
Over a third of respondents said they intend to leave their current role within the next two years, with the most common reasons related to a lack of satisfaction with their role or setting. Less than half expected to be working as an OT for over ten years. Whilst retirement was the most common reason given for leaving the profession, other reasons for leaving the profession were most linked to lack of satisfaction with their role, including lack of fulfilment, rates of pay and lack of opportunities for progression.
Many OTs said they’re passionate about their profession but frustrated their work settings don’t permit them to practice in a way that best uses their OT skills and expertise. Some linked this to a lack of understanding of the OT role by colleagues from other professions. Others blamed a lack of OTs in leadership roles within their organisations. Issues with increased demand, staff shortages across multiple professions and long waiting lists also meant some OTs were expected to ‘dilute’ their roles to cover others’ responsibilities, or to reduce their input so more people could be seen overall.
What should the OT workforce look like?
Occupational therapists as an allied health professional (AHPs), leadership and integration
Occupational therapists are one of 14 Allied Health Professions (AHPs), working across various sectors including health and care, education, academia, research, and the criminal justice system. As highlighted in the introduction, they are the third largest clinical workforce in the NHS but the smallest registered professional group in social care. The context provided by NHS England’s Chief Allied Health Professional and the AHP Strategy for England is crucial for understanding the role of OTs in councils.
Even with recognition and support from the Chief AHP, the extent to which NHS England and the supporting AHP infrastructure recognises and supports OTs in councils is reported to be variable. An OT in a leadership position in the council, with the capacity to engage, is one of the factors that can make a difference to ensuring that their specialism, and the role of adult social care, is heard within the NHS.
The necessity of strategic OT leadership in councils to enabling integration between health and care, ensuring there is the workforce needed to achieve a more sustainable, seamless, person-led, care experience and using the AHP architecture to best effect has been the finding of three sequential projects commissioned by the Chief AHP. Delivered through Health Education England, now the Workforce, Training and Education Directorate (WTE) and in partnership with the growing Principal and Strategic Lead Occupational Therapists Network (117 members at time of publication), a number of recommendations have come to fruition, including the inclusion of OTs in the LGA’s annual employer standards survey, in addition to social workers, but there is further work to do to realise the ambition for an integrated health and care workforce that optimises the use of OTs.
To enhance Equity, Diversity, and Inclusion (EDI) and improve accessibility to the OT profession, different routes into occupational therapy should be encouraged. This includes offering bursaries and training programs to attract a diverse range of candidates. By providing financial support and alternative pathways, the profession can become more accessible and inclusive.
The LGA is rolling out a recruitment re-set offer to councils and working with PCH to create a retention re-set tool for adult social care. These initiatives aim to address recruitment challenges and improve retention rates within the OT workforce. By focusing on both recruitment and retention a more stable and sustainable workforce can be built.
Agency usage is also a significant factor affecting service delivery and the permanent workforce. High reliance on agency staff can impact service continuity and increase costs. The LGA are currently working with ADASS to develop principles for agency usage to mitigate these issues and ensure better outcomes for service users and the workforce.
Workforce modelling and planning
Workforce planning for occupational therapists is led by NHS England and based solely on NHS data ie, modelling for OTs and student placements does not take account of the need for OTs in councils. This issue has been known for some time.
With the exclusion of council requirements for OTs, the NHS Long Term Workforce Plan modelled shortfalls in professions indicated that among allied health professions, OTs are one of five where shortfalls are expected to increase the most by 2036/37, with the education and training pipeline not keeping pace with expected demand. The Plan sets out ambitions to grow the OT workforce by 3.4 to 3.7 per cent, through training places, and to support OTs through increasing OT assistant roles. The Royal College of Occupational Therapists has drawn attention to the Plan’s lack of consideration to social care and capacity in this part of the system, particularly with an ageing population.
The Royal College of Occupational Therapists published a new workforce strategy in 2024, with a vision for an expanded occupational therapy workforce positioned to have maximum impact in improving people’s health and quality of life. By 2035 the ambition is for a workforce that is:
- confident and skilled in championing inclusion
- based primarily within communities
- positioned to focus on prevention and early interventions
- putting occupations at the forefront of their practice.
In addition to plans to improve workforce intelligence, RCOT seeking to support the optimal use of OTs, including in their local leadership role, and in demonstrating value and impact.
In the absence of a Government strategy for adult social care, the sector – including the LGA – has come together to develop one. This expects we will need an integrated workforce that focuses on personalisation, prevention (including avoiding people going into hospital) and wellbeing, and if people’s personal needs are to be met, more people in particular roles for example OTs are needed. The strategy also highlights the need for:
- Joint training, integrated teams, developing more clinical skills in social care and rewarding those skills and career development pathways between health and social care.
- Different roles and skills to support people with their mental health.
- Different roles and skills in technology, including technology-enabled care and AI.
In some councils, OTs in leadership and in practice roles, are already engaged in enabling these needs to be met; there is positive practice to build on.
Workforce intelligence
To enable an integrated health and social care workforce, a deep and detailed understanding of the local, regional, and social care workforce is crucial. More information is available from RCOT workforce strategy.
In the absence of this, some work has been completed, or is underway, to better understand the picture. This work is funded through WTE regional allocations, where the region has identified this is a priority; not all regions are doing this work.
West and East Midlands regional work to understand AHPs in social care
Recognising the diversity in social care delivery involving AHPs, this report aimed to scope the social care AHP workforce for both children and adult services in each ICS in the Midlands, describing service delivery models and funding streams used for staffing. It identified registered 594 OTs and 395 non-regulated assessors who complete OT interventions.
Issues impacting social care occupational therapy services across the region include pay disparities, unstable funding, overreliance on temporary positions and inconsistency in the measurement or evaluation of outcomes. Also, lack of recognition of the AHP’s skills and professional contribution could ‘lead to a continuation of a more reactive, and less professionally diverse system, where the cost benefits from prevention are not fully realised.’
To achieve the ambition to integrate workforce development programmes across ICS, it advocates for sufficient inclusive funding, and strong, sustainable AHP leadership in social care, alongside collaboration with clinical and care professional leaders in the ICS.
The principal and strategic lead occupational therapist perspective
Participants in this research, working in councils, shared their experiences and insight. This largely mirrors the findings of survey and regional work described earlier, and draws attention to issues associated with working in a council, and in adult social care in particular:
- Recruitment is a continual challenge, with associated costs including recruitment exercises, and the use of locums. Short term funding for posts is also not helpful.
- Lower rates of pay offered by some councils compared to the NHS, and a better pension offer in the NHS compared to local government, are significant factors, alongside fewer opportunities for learning and development (one of the four pillars of the OT profession’s practice) and career progression.
- Due to the financial situation of many councils, vacant OT posts have been removed from team’s complements.
- Located primarily in adult social care, the role and value of OTs is only understood in terms of assessments and waiting lists, not outcomes; council IT systems do not capture relevant data and OTs spend time trying to find workarounds
- There can be lack of parity with registered social workers in councils; there can be a perception that only social workers can undertake a Care Act assessment; such is the demand on OTs, it can be more difficult for them to gain necessary experience in areas that would enable them to progress to management roles.
- Not all councils have an occupational therapist in a senior and leadership role with capacity to engage in projects and service improvement and transformation; these roles have been recognised as effective by DHSC. This limits opportunities for councils to:
- Ensure that OTs in councils can practice effectively and safely.
- Learn from what OTs are seeing in the community and in their interactions with service users, including the impact of the NHS on the population’s demand for council services and associated costs.
- Use their professional skills to contribute more to local outcomes, including through joint work with other council services, the NHS, the voluntary and community sector.
- Ensure the council and adult social care is understood by other AHPs, and more widely within the NHS, including by other OTs.
Case studies
Annex A: Approach to the research, and limitations
Approach adopted
Participation of occupational therapists
- All OTs engaged in the research have been supportive, and keen to engage as far as their availability and capacity has allowed.
- The work began in June 2024: a workshop was hosted on the 22 July, attended by 53 people, located in 49 councils.
- Individual conversations have been held with people who could not attend (11 people).
- Four follow-up discussions were hosted in the first and second weeks of September, attended by 41 people from 21 councils.
- Those who have participated are primarily located in and/or work alongside council adult social care.
- The summer holiday period limited initial engagement and follow-up with those who attended or expressed an interest in the work.
Policy review
- A desktop review and 18 policy conversations (Annex B) followed the initial group discussion with OTs.
- Together these explored existing evidence and policy in support of optimising the role of OTs in council services, and emerging opportunities considering the new government, the future of adult social care and the NHS.
Limitations
- This is a time-limited and exploratory piece of research. It was not possible to do justice to the role of OTs in all council services.
- Further research is recommended to explore the contribution OTs in councils make, and what’s needed to optimise this, in relation to:
- Children and young people, including in education, for children with Special Education Needs and Disabilities (SEND), and young people as they leave education and transition to adulthood and independence.
- People who are economically inactive, particularly owing to ill-health or health conditions.
- People experiencing multiple and severe disadvantage eg, people in contact with the justice system.
- The RCOT acknowledges a gap in the evidence of the value of occupational therapy, particularly to make the case for further investment. The College’s workforce strategy, innovation hub and planned research and innovation strategy all seek to address this.
- The UK Allied Health Professions Public Health Strategic Framework 2025-30 also acknowledges a challenge in demonstrating impact; one of the framework’s five goals is for AHPs to be able demonstrate their contribution to improved outcomes, using data and intelligence from evaluation and research to guide decision-making, design new models of care and show impact.
- OTs engaged in this research reiterated the challenges in demonstrating their impact: these, and recommendations, are discussed in the report.
- In this work it has been difficult to secure new in-depth case studies, an experience shared by other stakeholders for reasons related to wider challenges experienced by councils and services working in the community. These include:
- The capacity of OTs to generate case studies in addition to their day-job.
- The impact of preventive approaches is harder to measure.
- The work of the OT and related interventions are person-led, not standardised.
- Outcomes require a longer-term approach to learning and evaluation than is currently available – and longer-term, stable, funding in the approach/interventions to begin with.
- Local datasets do not adequately capture the OT input, outputs and outcomes.
- For this report, some examples of the evidence of the value of occupational therapy in councils has been reproduced, with permission.
Annex B: Stakeholders engaged
| Contact | Organisation |
|---|---|
| Shiva Sapra | Department of Health and Social Care |
| Victoria Bennett | NHS England |
| Priya Oomahdat | NHS England |
| Nicola Gitsham | NHS England |
| Linda Hindle | Office for Health Improvement and Disparities |
| Lauren Walker | RCOT |
| Joe Brunwin | RCOT |
| Paul Smith | Foundations |
| Rachel Russell | Foundations |
| Antony Tucker & Jack Sansom | NHS Confederation |
| Ian McCreath | TLAP |
| Suzannah Young | Nat Housing Federation |
| Matt Hibberd | LGA |
| Mairead Rooney and Nicola North | LGA |
| Hazel Summers | Health and Care Partners, LGA/ADASS |
| Lynne Bowers | ADASS West Midlands Associate |
| Professor Mary Lovegrove | Allied Health Solutions |
| Sally Burns | DPH, West Northants |