This section shares key insights and learning gained from the delivery of the Support Programme. It reflects on what worked well, the conditions that enabled progress and the challenges encountered and resolved. The aim is to support continuous improvement by informing future practice both within participating systems and more broadly across the sector. The insights presented draw on both our internal reflections and key insights into the impact of the Support Programme, its strengths and areas of development, and from the independent evaluation of the Programme by IPSOS.

The key insights from IPSOS on supporting systems are:
- Sustaining change: several of the desired impacts of the Support Programme are grounded in the aim of sustaining improvements in the longer-term. The evaluation found that for systems, the prospect of sustaining change after the conclusion of support delivery was often challenging. Systems often acknowledged the value of the support, and the recommendations provided, but struggled to translate these into sustained action. The day-to-day pressures of existing workloads and more immediate operational demands consumed available time and resources, leaving little capacity for the ongoing effort required to sustain changes within existing systems. This was particularly true in systems lacking dedicated staff or funding for transformation work. The short-term nature of the support itself exacerbated this challenge, creating a ‘cliff edge’ where some systems lost momentum and focus after the initial burst of activity.
- Tailor the support offer to system needs: Offer more bespoke support tailored to individual system needs and maturity levels (defined as having aligned priorities and a shared understanding of BCF priorities and issues). Avoid generic offers that do not address specific challenges or account for systems to provide direction and focus for the support. Offer support that is seen as a proactive, positive offer for ambitious systems.
- Facilitate peer learning and networking: Establish peer learning opportunities and networks to share best practices and learn from each other's experiences. Showcase examples of successful support projects and use this as an opportunity to positively frame the Support Programme as something to enhance success as opposed to an offer for struggling systems.
- Focus on leadership and behaviour change: Emphasise the importance of leadership, culture, collaborative working, and behaviour change in driving successful implementation via support offers. Provide specific support and resources to foster these elements, possibly as a standalone element of the Support Programme.
- Targeting support: The Support Programme delivers a high number of small support projects across many systems. Its impact on individual systems would likely be greater if it focussed on longer-term, intensive support across a smaller number of more stringently selected systems. However, consideration should be given to how they should be selected to balance offering support to systems which need it most with offering support to systems best able to make changes as a result.
- Capacity building: Systems often lack the capacity to implement recommendations, both in terms of staffing and expertise. Ongoing support and resources are needed to address this.
- Capturing the long-term impact of support: To fully understand the long-term impact of support projects at an individual system level, more robust, longitudinal evaluations would assess the programme's impact more comprehensively.
- Focus on implementation: While the Support Programme has achieved positive outcomes in some areas (e.g. building consensus, improving relationships, improved system understanding of specific issues), there is a need for greater focus on implementation and tangible change in the medium to long term. Systems need support to translate plans into action and achieve measurable improvements in areas like discharge planning and capacity management.
The insights from the Support Programme are structured around the four conditions of success for integrated health and care systems: quality of relationships, quality of data-driven decision making, quality of effective actions and planning and quality of measurable results and sustained improvement.
Key insights on the quality of relationships: the foundation stone
- Support from the Programme has surfaced relationships between system leaders which are fragile. In some cases, behaviours are not conducive to building and maintaining trust. Relationships are conducted against the backdrop of financial, demand and workforce pressures.
- The National Better Care Fund’s team’s Planning and Assurance (P&A) Survey highlighted an emerging tension in system relationships regarding predominance of acute hospital influence, and a desire to shift resources to community health provision.
- Technical improvement support has been enhanced when it has been accompanied by support for leadership around collaborative working, decision making and governance. This focuses on embedding trust between senior leaders and strengthening governance infrastructure to sustain these ways of working.
- The transparency and consistency of funding decisions have a particularly significant impact on relationships between system partners. We have observed that the cost pressures on ICBs are a recurrent cause of weakening relationships.
- In acute settings, in terms of relationships amongst frontline staff, there has been a loss of integrated team working since the move to remote working at the onset of the COVID-19 pandemic, leaving hospital wards less skilled to deal with discharge well without social worker input. Frontline acute staff have expressed a desire to have more knowledge of social care available to them, as well as the constructive challenge social workers or trusted assessors can provide in decision making.
- In other cases, rather than relationships having broken down, relationships are weak because they have not been built up in the first place.
- Colleagues in health and social care are committed to doing their best for the people they serve. There is widespread recognition of the value of both sectors working more closely together, but structures and processes do not always enable colleagues to do so.
- A consistent theme from senior leaders involved in the scoping diagnostic support undertaken by the Programme in 17 systems was that it was rare to come together in this way to discuss causes of whole system challenges, work on potential solutions, and have a safe space to have the difficult conversations.
- The Programme delivers a four-module Discharge to Assess in-house support offer. An important feature of the offer is a set of workshops which brings health and social care staff together to review discharge decisions for a large number of cases from their system. Participating staff have expressed what a rare opportunity the offer provided for teams to come together in a multi-disciplinary setting to review former cases and reflect on whole system improvement.
- Survey data from the six pilot systems which received this offer showed a higher level of trust in senior leaders within the organisation of the respondent than across their health and care system as a whole, who were only trusted by a minority of respondents. In low trust environments, organisations are less likely to take on ownership and risk of actions which could lead to improvement for the whole system.
- Though the introduction of ICSs has been welcomed, senior turnover in the transition from CCGs has meant that some relationships which were adding significant value have been lost, with a loss of historic knowledge and organisational memory. Added to this, it is important to recognise new complexities of commissioning, now involving provider collaboratives as well as ICBs and local authorities.
- Systems have identified having to respond regularly to varied asks from central government and NHS bodies impacts on time available to engage with system partners more proactively. The P&A Survey suggested that BCF publication and planning timeframe challenges can hamper partnership working and collaboration. The D2A Support Offer highlighted that the participating systems were more likely to dedicate analytical resource to the upkeep of national performance reporting than strategic commissioning and decision support. This is inadvertently leading systems to narrowly focus on challenges and symptoms in isolation rather than seeing and understanding all the interrelated parts and taking a whole system approach. Excessive requests for data can lead to the behaviour of treating data gathering as a paper exercise, disconnected from wider improvement efforts.
- Responding to the P&A Survey, the National BCF Team reflected that publication and planning timeframes often do not allow the BCF locally to achieve its full potential, or allow for thinking and planning time, and a robust project management approach to developing new ideas and services. To promote innovation, systems identified the need to focus less on rigid reporting and shift the emphasis towards creating the right conditions for enabling good practice and innovation.
- In many systems, hearing and understanding the voice of people with lived experience is not built into business as usual. The Voice of the Person module of the D2A offer, which consists of a series of service user interviews, proved to be the most challenging for systems to undertake successfully. For service organisations such as health and care, user feedback is critical to improvement. Systems lack infrastructure and governance to engage in this feedback as priority and standard practice.
Key insights on the quality of data-driven decision making: the system think tank
- Systems list differing governance, funding and accountability arrangements between local government and the NHS as barriers to integrated working. Where relationships are not strong or the governance infrastructure needed to sustain them is underdeveloped, systems can revert to considering issues in isolation, from the perspective of individual organisations. This is especially true for systems experiencing major pressures.
- Systems which rush to action in this way often find that their efforts to resolve an issue offers temporary relief, but that the issue recurs in the future, or re-emerges in another part of the system. Symptoms are being treated, rather than the underlying conditions.
- Repeated feedback from systems has been that the Support Programme offers value by creating space for holistic consideration of complex issues.
- Services can struggle to track costs across patient discharge pathways. This weakens financial governance, making it harder to set budgets and monitor the financial impact of long lengths of stay.
- The Better Care Fund part-funds services, which can make it complex to dissect, monitor schemes within BCF Plans and evaluate whether they are fit for purpose. Colleagues responding to the P&A survey said that in their systems the BCF has been funding the same activity (including historic or statutory services) for many years so isn't viewed as ‘new money’, which often leads to funding ‘more of the same’ type of activity and means limited funding for innovation or 'new' services or initiatives each year. In many systems, there is minimal capacity deployed to oversee the BCF. This process requires more oversight and leadership at the senior level.
- In many systems, the role and contribution of strategic commissioning in decision-making process remains unclear. Commissioning, financial and operational insight are not joined up.
- One of the most prominent examples of siloed thinking across systems has been the use of data to support decision making. Systems are data and information rich, but it is spread across different organisations, and it can be unclear what decisions (strategic, operational or commissioning) the data is designed to support. Data availability, consistency and reliability are entrenched and ongoing challenges.
- There are often multiple data solutions in use in systems. Despite systems having powerful dashboards, data frequently is not captured in one place. This can mean collation is laborious and analysis is time-consuming, with systems often working from multiple spreadsheets across multiple teams.
- The Programme has found a consistent capacity gap around manipulating cross-system data to provide leaders with meaningful information which supports decision making from a whole system perspective.
- A significant focus of funding partners and the Programme was on improving the ability of systems to forecast capacity and demand. Our observation has been that in many systems, collation of this data was being treated as an information gathering exercise to fulfil reporting requirements, instead of a basis for collective planning.
- One of the areas most affected by mutual misunderstanding is intermediate care. Efforts can be made to improve performance of individual services in siloes, such as specific bed-based schemes, when they are in fact interrelated and interdependent and part of the same intermediate care process. There is a need to reframe the approach to intermediate care. The ‘Business Case for Home-Based Intermediate Care’ (HBIC) published by the Programme demonstrates that investing in HBIC is one of the most cost-effective measures available to the sector.
- Staff can also be unclear about what intermediate care services are available locally, sometimes because there has been a number of changes to how intermediate care is provided over time. This makes staff more likely to recommend bedded care when a better alternative may have been available.
- We have regularly encountered misunderstanding and misinterpretation of national policy and guidance in the delivery of support around Discharge to Assess, Home First, intermediate care and BCF funding. This leads to variation in how the guidance is being implemented.
- In each of the systems that participated in the D2A Support Offer, there was significant confusion about the definitions of Pathway 1 and 2, as well as variation in the use of terms like “discharge to assess”. In some places, “discharge to assess” was a byword for the use of interim placement beds as an intermediate care offer, whereas the term “D2A bed” was used when someone was discharged to empty a hospital space, whether the bed-based care offer was appropriate or not. The expectation from NHS clinical staff seemed to be that Council partners would pick people up from these settings and make a decision about long-term need in intermediate settings, even when there was no clear mechanism to report that people had been discharged this way.
- The main causes of non-optimal pathway usage identified during the pilots were risk aversion by staff, and preference for bedded care by the person or their family. Staff can only have the confidence to recommend care at home and respectfully challenge patients and families if they are themselves confident in the underlying principles of Home First.
Key insights on the quality of effective actions and planning: the strategic blueprint for the system
- The quality of action taken to improve services by systems and support providers is a result of the quality of relationships and thinking. It is also dependent on an ability to translate this into actionable plans.
- While systems have valued the support and the recommendations provided by the BCF Support Programme, they struggle to translate these into implementation plans and sustained action. Some systems have said that they lack dedicated staff or funding for transformation work. The actionable plans need to have a mix of short-term actions to create momentum for change and address immediate priorities, and longer-term plans to ensure sustainability. There can be a danger that the short-term crowds out longer-term issues. Limited joint planning for long-term shifts such as demographic changes will keep systems stuck in a cycle of crisis response.
- Lack of clarity on funding flows and cost drivers across organisational boundaries leads to less effective financial planning, affecting investment across health and social care.
- One area for action is patient flow. Where systems do not have a joint understanding of patient flow through discharge and intermediate care processes, it is inevitable that management of flow will be a challenge. A lack of real-time visibility into resource capacity, demand and workforce skill mix stops systems from optimising schedules and staffing to match patient volumes. Another area is capacity. Systems will find it difficult to achieve optimum capacity unless commissioning acts on what emerges from analysis of demand and flow.
- Within individual systems, partners are not always appropriately sighted and invited into the governance of improvement practice being conducted in other parts of the system. This makes it much harder for practice to be scaled up across systems. There is a gap in oversight and programme management of the range of improvement efforts underway in different parts of the system at any one time.
- Improvement support is a crowded arena, with national and regional bodies and private consultancies seeking to deliver support to systems. This sometimes takes place without synergy and co-ordination between providers. Systems have expressed that this can distract and overwhelm them, undermining the impact of the support offered.
- There is an enormous amount of good and innovative improvement work taking place in the different services and organisations across health and social care systems in England, but not evidenced effectively. It is often undertaken in siloes, limiting the opportunity of scaling up successfully and delivering maximum benefit. There is a keenness among systems to learn from other systems, with requests often made to the Programme for relevant good practice to be shared. It is important to remember that good practice examples from other settings will only be helpful if a system has the time, capability and capacity to understand benefits and evidence, adapt and make the case and embed the practice in their own setting. A behavioural science approach needs to be adopted to support systems to become innovators and early adopters of best practice. (ref: Diffusion of Innovation (DOI) Theory, developed by E.M. Rogers in 1962).
- Improvement support follows a cycle, the Plan, Do, Check, Embed model often used in quality assurance. If results are not studied collaboratively, learning cannot be applied coherently. The success of improvement is too often being judged in siloes, using indicators geared towards individual services. We have found that where change programmes take place without alignment, long-term planning or reflective practice, this leads to inconsistency of decision-making among senior leaders and confusion among frontline staff.
- Under the current Support Programme contract with DHSC, the support offered by the Programme has been concentrated in the top right half of the cycle, ’Plan’. We increasingly have received requests from systems for support for the duration of the bottom half and top left, ‘Do, Check and Embed. The Programme has met these requests in three systems around Care Transfer Hubs. Implementation support of this kind would be enabled by supporting systems on a longer-term basis to establish and embed sustainable action.
Figure 5: Plan, do, check, embed
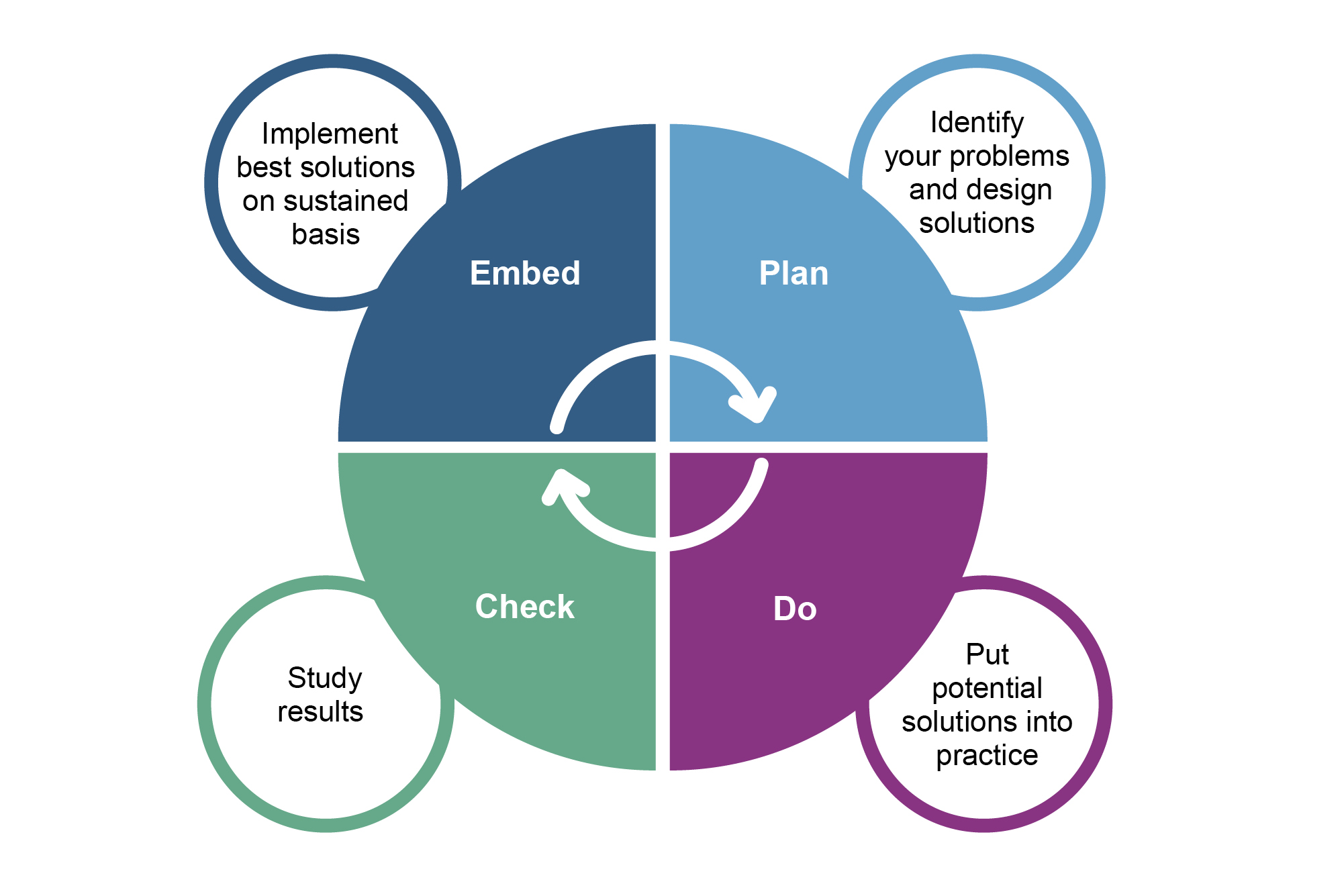
The diagram above shows the steps to Plan, Do, Check and Embed: identify your problems and design solutions; put potential solutions into practice; study results; and implement best solutions on sustained basis.
- Actions to improve services are ultimately delivered by the workforce. Across support offers, the Programme has encountered high vacancy rates, and reliance on temporary staff. In addition, we have seen strict workforce rules and lack of flexibility, fixed staffing ratios, and complicated approval processes.
- Capacity and demand forecasting capability is limited for workforce utilisation, as it was found to be for the forecasting of service use. Taken together, these challenges are leading to an inability to flex workforce resources across systems to match evolving needs, and to adapt to fluctuations in demand.
Key insights on the quality of measurable results and sustained improvement: the building of momentum
- In the Core Theory of Success for Learning Organisations, Kim stresses that the quality of results are the direct consequence of the quality of relationships, thinking and actions. This is in line with the findings of the Programme.
- Risks to quality of thinking include rigid mental models or mindsets, groupthink, lack of critical reflection and resistance to new ideas. If assumptions are either flawed or outdated, they will lead to learning the wrong lessons and poor decision making.
- Systems are frequently data rich, with good levels of and information and intelligence. However, poor decision processes can derail the delivering of good outcomes. Decision making based on assumptions rather than starting from the evidence, dominance of the ‘loudest voices’, and not engaging with the frontline or diverse perspectives can be key barriers.
- Where robust decisions are taken, how strategy is translated into execution is just as important. This can be held back by disconnection between planners and implementers in a system, misaligned actions, or lack of ownership of actions.
- Systems are not always able to capitalise on and benefit from learning from past experiences. Behaviours associated with this include siloed communication, struggling to see the bigger picture, and avoidance of blame. A culture which does not support open dialogue, research, testing and learning will lead to risk aversion and can stifle quality improvement.
- As well as being important in their own right, quality of results matter because they reinforce the quality of relationships, starting the cycle again. Partners see the value of working collaboratively, which encourages them to continue to do so.
- When there are gaps in the four conditions of success identified by Kim, systems can enter a cycle of rushing to action, chasing quick wins and not addressing root causes. Pressure for short-term results, leadership turnover and workforce challenges can all incentivise this approach over sustainable, systematic change.
