
Foreword
Everyone deserves the same opportunities to lead a healthy life, no matter where they live or who they are.
But in England today there is almost a 20-year gap in healthy life expectancy between the most and least affluent areas of the country. It is a stark symbol of social injustice that those living in the most deprived communities spend more years in ill health and die sooner.
Closing this gap is one of the biggest challenges we face so we must keep reinforcing the message that health is about much more than healthcare or the choices we make about our diet or whether we exercise, smoke or drink alcohol.
In fact, the best way of ensuring a long life in good health is to have a good start in life, a good education, a warm and loving home and an income sufficient to meet our needs.
And because we understand that reducing health inequalities is about jobs that local people can get, decent housing and preventing people becoming isolated, it follows that we also recognise that places and communities have the most critical role to play.
If we all work together to get this right our neighbourhoods are more productive and prosperous, and we support and encourage people to use the NHS and social care less and later in life, to stay well for longer, and when unwell to stay in their home for longer, and to stay in work for longer. Health and wealth are truly two sides of the same coin.

Councillor David Fothergill
Chairman
LGA Community Wellbeing Board
Introduction
Health is not just about the length of life we live, but also the quality of life – the gap in healthy life expectancy (years lived in good health) between the most and least deprived areas of England was around 19 years (change to 20 years)for both males and females the gap in life expectancy is growing.
The extra cost to the NHS and social care from health inequalities have been calculated as £5 billion a year in greater hospitalisations alone.
Health inequalities reduce employment and productivity, which costs national and local economies – acting on health inequalities is, therefore, an investment for England’s national and local economies.
Health inequalities are not caused by one single issue, but a complex mix of environmental and social factors which play out in a local area, or place - this means that local areas have a critical role to play in reducing health inequalities.
Addressing the wider determinants of health through a life course approach is important for achieving impact at the level of population health - rather than at the individual level.
The following guide offers a high-level overview for all councillors and officers of key issues with regard to understanding and tackling health inequalities.
Definition of health inequalities
Health inequalities are unfair and avoidable differences in health across the population, and between different groups within society. Health inequalities arise because of the conditions in which we are born, grow, live, work and age.
These conditions influence our opportunities for good health, and how we think, feel and act, and this shapes our mental health, physical health and wellbeing.
Health inequalities have been documented between population groups across at least 4 dimensions, as illustrated in Figure 1 below. It is important to note that these are overlapping dimensions with people often falling into various combinations of these categories.
Figure 1
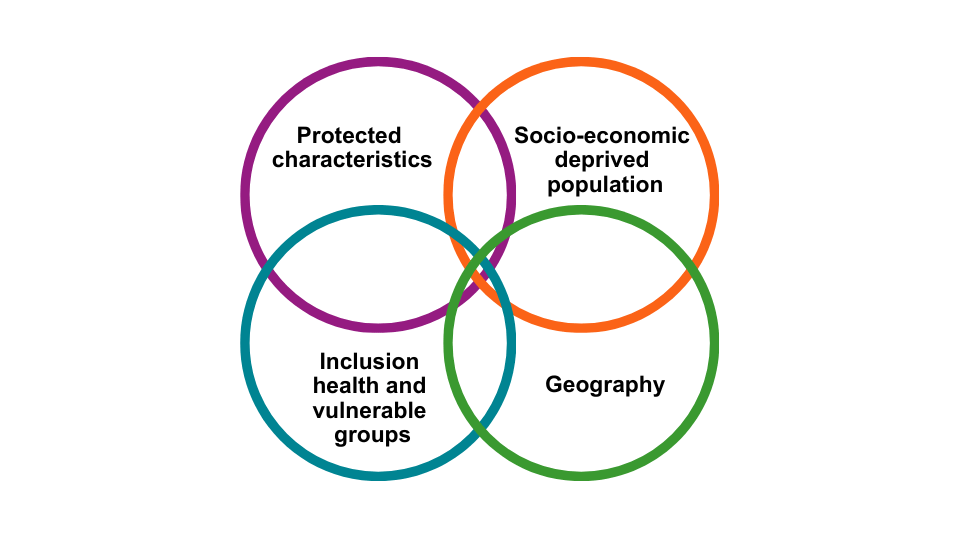
Examples of the characteristics of people or communities in each of these groups are below (this is not an exhaustive list):
- Socio-economic status and deprivation, for example, unemployed, low income or people living in deprived areas. This could include poor housing, poor education as well as unemployment.
- Protected characteristics – Religion/belief, age, sex, race, sexual orientation, gender reassignment, marriage and civil partnership, pregnancy and maternity and disability.
- Vulnerable groups of society, or ‘inclusion health’ groups, for example, vulnerable. migrants; Gypsy, Roma, Boater and Travellers, as well as homeless people, sex workers and offenders/former offenders.
- Geography, for example – urban, rural or coastal areas, built and natural environment and levels of social connectedness.
The effects of inequality are multiplied for those who have more than one type of disadvantage.
Equality, equity and removal of structural barriers
Figure 2 below illustrates the characteristics of people or places associated with differences in health outcomes.
Figure 2
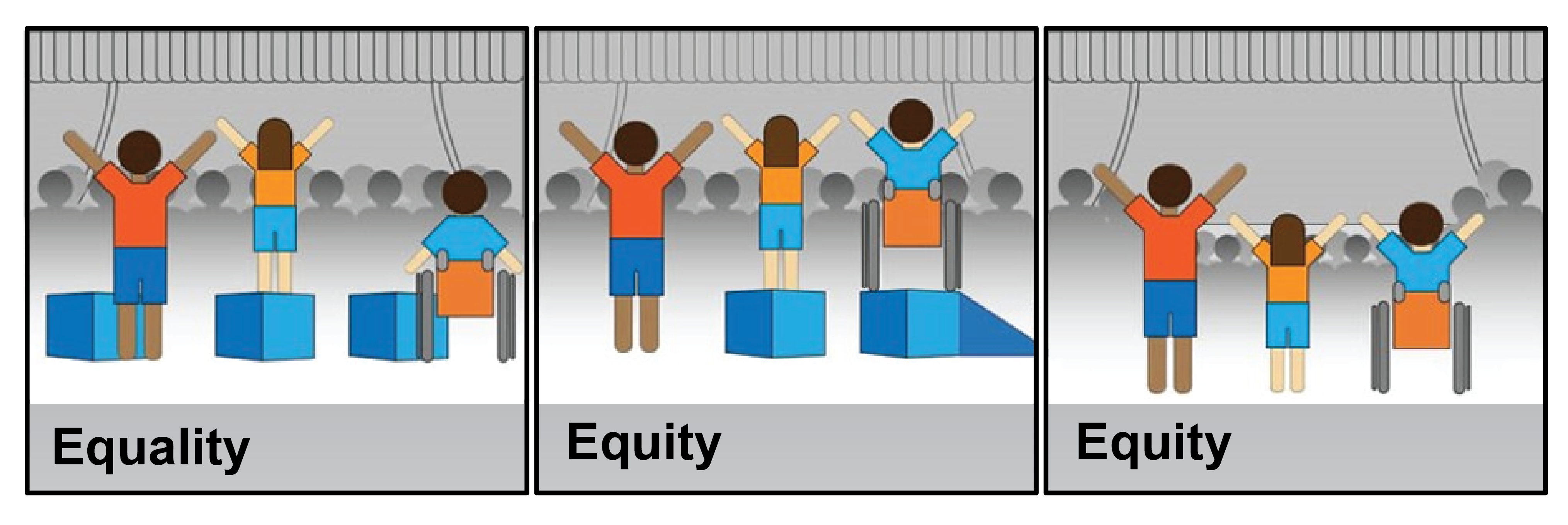
Some other key terms in health inequalities and health disparities are:
- Equality: We want everyone to have equally good health. However, the term ‘equality’ is sometimes used to describe equal treatment or access for everyone regardless of need or outcome.
- Equity: We want fair outcomes for everyone. What is important is addressing avoidable or remediable differences in health between groups of people. Figure 2 demonstrates that, to achieve health equity, some groups may need more or different support or resources in order to achieve the same outcomes. Ideally, the barriers to good health would be removed for everyone, so adjustments wouldn’t be required – however, this is not always possible.
- Equal outcomes: Ensuring everyone can access services equitably (that is according to need). To achieve this, consideration needs to be given to access to information, services and support. Central to this is enabling people to access the right service at the right time for them, reducing variation in the avoidable use of urgent support such as accident and emergency services through better access to preventative care.
Economic case for acting on health inequalities
There are many reasons to come together to find solutions at a national and local level to break the cycle of entrenched health inequalities in England. As many of these inequalities are avoidable, the moral case cannot be overstated.
There are also economic reasons for action. The high burden of disease in deprived areas generates higher use of health and social care services, higher unemployment, and lower productivity.
The Marmot Review estimated that health inequalities cost society £31 billion in lost production, in 2010 prices. Whilst this is a national figure, it is in local jobs and economies where this impact is borne out.
The higher burden of disease experienced by women living in the most deprived neighbourhoods costs the NHS 22 per cent more per person than women living in the least deprived neighbourhoods, despite having shorter life expectancy (or £400 per person per year in secondary care costs).
For men, this figure is 16 per cent per person (or an additional £300 per person per year in secondary care costs). This results in an additional spend of £4.8 billion per year, almost 20 per cent of the total hospital budget, without taking into account additional costs, including social care provision.
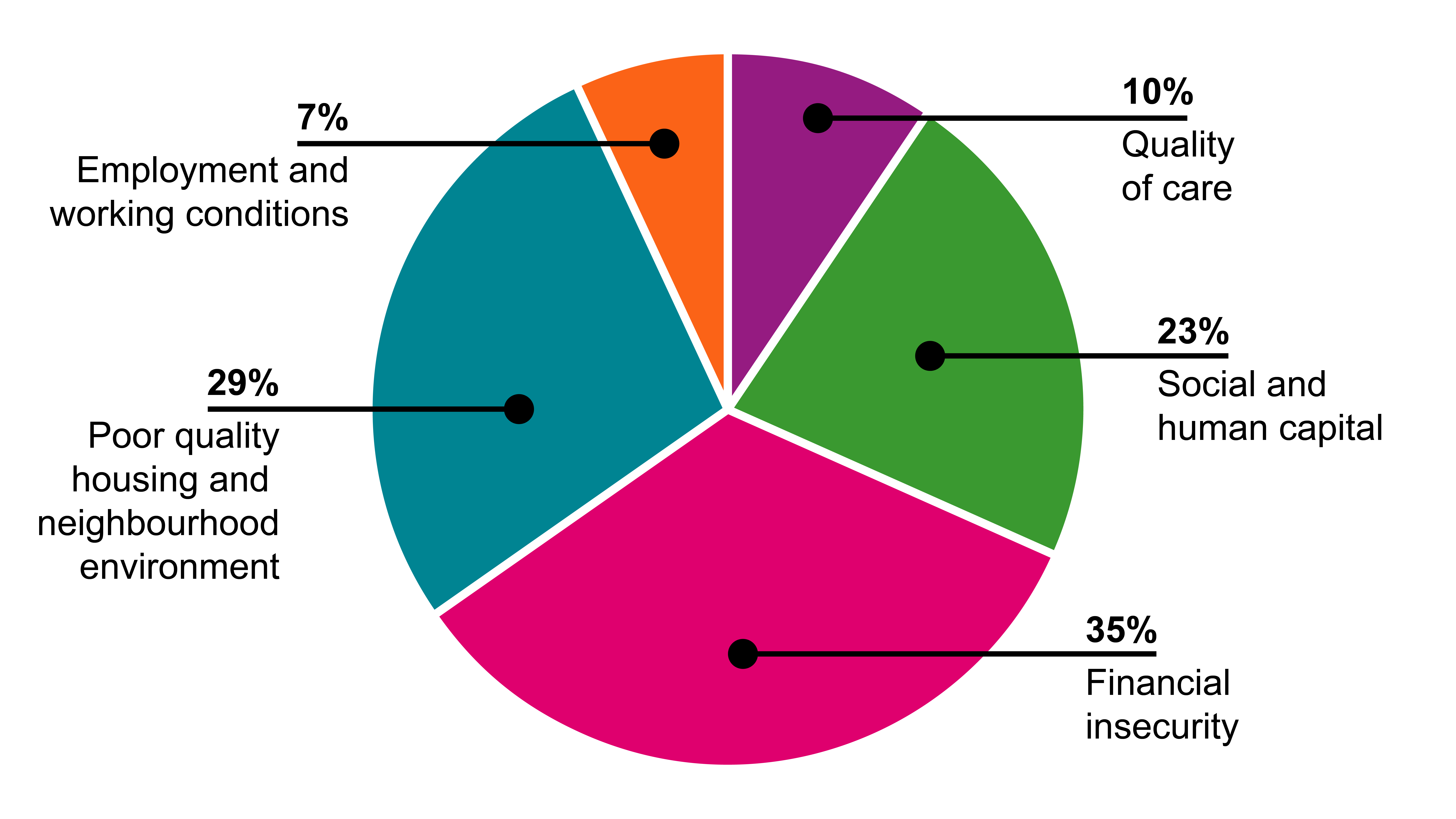
Causes of health inequalities
The causes of health inequalities are fundamentally linked to social, political, and economic factors that influence the distribution of power, money, and resources between different population groups and social classes. A report by the World Health Organization links them to the five key factors below. Quality of care accounts for just 10 per cent of health inequalities.
Figure 3
The health conditions responsible for poor health and health inequalities can change over time. But as new conditions emerge, inequalities in these usually arise very quickly; as seen for example during the COVID-19 pandemic. Low income, ethnic minority and disadvantaged populations were more likely than other groups, to contract COVID-19. They were also more likely to experience severe disease and suffer the wider effects of the pandemic. This example demonstrates the fundamental causes. These groups were less able to protect themselves, due to inequalities between populations in power and resources.
Public Sector Equality Duty
The Public Sector Equality Duty set out in the Equality Act 2010 applies to all public bodies and all those that carry out public functions.
The protected characteristics covered by the duty are:
- age
- disability
- gender reassignment
- marriage and civil partnership
- pregnancy and maternity
- race
- religion or belief
- sex
- sexual orientation.
Public bodies are required to have due regard to the need to:
- eliminate discrimination, harassment, victimisation and any other conduct that is prohibited by or under the Equality Act 2010
- advance equality of opportunity between persons who share a relevant protected characteristic and persons who do not share it
- foster good relations between persons who share a relevant protected characteristic and persons who do not share it.
Inclusion health
Inclusion health is a ‘catch-all’ term used to describe people who:
- are socially excluded
- typically experience multiple overlapping risk factors for poor health (such as poverty, violence and complex trauma)
- experience stigma and discrimination
- are not consistently accounted for in electronic records (such as healthcare databases).
These experiences frequently lead to barriers in access to healthcare and extremely poor health outcomes.
Deprivation
Deprivation describes a wide range of living conditions that impact on the lives of individuals and communities. People may be considered to be living in poverty if they lack the financial resources to meet their needs, whereas people can be regarded as deprived if they lack any kind of resources, not just income.
The Index of Multiple Deprivation is the official measure of relative deprivation in England that measures 7 domains of deprivation when combined and appropriately weighted. These are:
- income
- employment
- skills training
- crime
- barriers to housing and service
- living environment
- health deprivation
- disability.
Geography
Health disparities and health inequalities are not spread equally across England. There are local variations in the concentration of pre-existing health conditions and chronic disease in certain geographies between different areas. Alongside and contributing to driving these are variations in protective factors, such as:
- living in a strong community
- access to green space
- the impact of living in specific geographies, such as coastal communities.
Why take action on health disparities and inequalities
Health disparities and health inequalities impact on the physical and mental wellbeing, and the life chances of the individuals and groups most affected. Alongside the individual human costs, disparities and inequalities impact on society as a whole.
Prior to COVID-19, health inequalities were estimated to cost the NHS an extra £4.8 billion a year, society around £31 billion in lost productivity, and between £20 and £32 billion a year in lost tax revenue and benefit payments. Health is therefore a major determinant of economic performance and prosperity.
Consequently, taking action on health inequalities:
- improves the quality of lives of individuals
- reduces cost to the NHS and social care system of treating and caring for people with preventable conditions
- benefits the wider economy.
How can we reduce health inequalities?
To effectively address health inequalities, action is needed at three levels: undoing the fundamental causes, preventing wider environmental influences, and mitigating individual negative impacts. This means tackling the root causes like poverty and lack of power, preventing harmful environments, and addressing the individual effects of these inequities.
Three levels of action are needed to address health inequalities:
- undo the fundamental causes
- prevent harmful wider environmental influences
- mitigate (make less harmful) the negative impact on individuals.
Undoing the fundamental causes
- Addressing the root causes of health inequalities, often referred to as 'upstream' interventions.
- This involves tackling issues like poverty, lack of access to quality education, housing, and employment opportunities.
- Examples include implementing policies that promote a living wage, redistribute power through community engagement, and address systemic racism and discrimination.
Preventing wider environmental influences
- Focusing on preventing harmful environmental factors that contribute to health inequalities.
- This includes addressing issues like air pollution, unsafe housing, lack of access to healthy foods, and inadequate public transportation.
- Examples include promoting healthy food environments in schools and workplaces, investing in affordable and sustainable housing, and improving access to public transit.
Mitigating individual negative impacts
- Focusing on mitigating the negative impacts of health inequalities on individuals.
- This involves providing access to quality healthcare, addressing individual health behaviours, and ensuring that marginalized groups have access to necessary support services.
- Examples include expanding access to preventative healthcare, providing mental health support, and ensuring equitable access to healthcare services.
By addressing all three levels, a comprehensive strategy can be developed to reduce health inequalities and improve the overall health and well-being of all individuals, particularly those who are most vulnerable.
Health behaviours
The ability of individuals to lead healthy lives is influenced both by the wider determinants of health, and by individual factors (health behaviours) associated with people’s opportunities and experiences.
The main behavioural risk factors for poor health – smoking, poor diet or excess weight, physical inactivity and high alcohol consumption – follow the same pattern of uneven distribution as the wider determinants of health, indicating that there is a relationship between an individual’s likelihood of smoking, eating healthily, physical inactivity, and their social and environmental circumstances.
Linked to health behaviours, the concept of ‘health literacy’ refers to people having the appropriate skills, knowledge, understanding and confidence to access, understand, evaluate, use and navigate health and social care information and services. Improving health literacy by supporting patients to engage in shared decision-making can help to reduce health inequalities by empowering and enabling people to navigate individual and societal barriers to improving their health and managing health problems.
The National Institute for Health and Care Excellence (NICE) guideline on shared decision-making describes how to make it part of everyday care in all healthcare settings.
Six priority actions
1. Have a clear vision and strategy with measurable goals, co-ordinating action at all levels (for example, across organisations or professional boundaries) with a clear focus on priority groups
Ask yourself:
- What is your vision? What are you trying to achieve?
- What would success look like for you or your organisation?
- Do you have a clear strategy and plan for achieving your vision?
- Do you have the right resources, and a timeline and plan?
- Who else could be involved?
- Is there a system, organisational or professional plan or guidance?
- Do you know your priority groups?
- Have you identified SMART (specific, measurable, achievable, relevant and time-bound) goals and measurable targets?
- Are your plans joined up across organisations or with other teams?
2. Put in place effective system leadership and accountability for action on health inequalities
Ask yourself:
- Who leads on action on health inequalities and health disparities?
- What’s your leadership role (whatever your level) – for example in your team, profession, organisation, multi-agency group, sector or network?
- What do you do to support others to take a leadership role?
- What does your organisation expect of you or others in respect of action on health inequalities? How are people held to account?
- Are you driving changes using quality, service improvement and redesign methodology including Appreciative Inquiry?
- Are you involving and co-producing change with those who are experiencing healthcare inequalities through engaging communities in design, implementation and evaluation?
3. Use data and evidence systematically to identify root causes, effective solutions and assess progress
Ask yourself:
- What information do you have to identify the problem you’re trying to address?
- What’s the scale of the problem and the root causes?
- How do you know that your planned action is likely to be effective?
- How will you know when you’ve achieved your goal or outcomes?
- How can you contribute to data collection – are you systematically recording health inequalities and equality data in your routine practice?
4. Ensure you or others have the knowledge, skills and capability to embed action on health inequalities as a core part of all roles
Ask yourself:
- Do you, your team or organisation have the knowledge, skills or training to take the required action?
- How could you acquire these?
- Who else could help?
- What’s included in job descriptions?
- Have you considered health literacy and shared decision-making? Do clients have the appropriate skills, knowledge, understanding and confidence to access, understand, evaluate, use and navigate health and social care information and services?
5. Use systematic assessment tools
Ask yourself:
- Do you use individual and population needs assessments?
- What tools are available to support you in your work? For example, the Health Equity Assessment Tool (HEAT)
- Do you use a health in all policies (HiAP) approach?
- Where might you find information on assessment tools? For example, the tools and resources repository on the Health Inequalities Knowledge Hub?
- What do other systems or partners use?
- Have you undertaken an equality and health inequality impact assessment?
6. Undertake comprehensive engagement and involvement including magnifying community voice
Ask yourself:
- Are your plans informed by local communities or client groups preferences and needs, including consideration of health literacy?
- Has involvement and engagement been systematic?
- Do you use community-centred approaches?
- Have you considered the strengths of individuals themselves and communities, and built these into your conversations or programme?
- Do you work with community or community health champions?
- Do you use personalisation approaches such as Making it Real?
- Do you use NICE, and other guidance and tools to support community involvement?
- Have you considered how to listen and learn from communities?
Leaders make an important contribution to prioritising and embedding whole-system action to address health disparities and health inequalities.
As a leader, you can use your role to:
- Identify key strategic partnership and collaboration opportunities to support whole-system at scale action – for example, through ICS structures, primary care networks, health and wellbeing boards, local economic partnerships, community safety partnerships, and working with VCSE partners.
- Demonstrate your personal and organisational commitment to addressing health inequalities.
- Use your health, care, wider system and place leadership role to prioritise at scale, tackling differences in health outcomes first and fastest.
- Use the well-led framework for health inequalities leadership in strength-based social care.
- Review all the resources and content in place-based approaches to reduce health inequalities and complete Tool A with partners for your system or place.
- Undertake a needs assessment – for example, a joint strategic needs assessment to identify priority need, issues and actions at sufficient scale to make a difference, setting goals and targets to measure impact.
- Use HEAT and HiAP approaches to take account of health inequalities in all decision-making.
- Embed community-centred approaches in organisational and system-wide ‘business as usual’.
- Use your organisation’s role as an anchor institution – for local councils, this could involve: purchasing more locally and for social benefit, widening access to quality work, using buildings and spaces to support communities, working closely with local partners, reducing environmental impact.
- Review the SCIE resources on addressing health inequalities.
Professional resources and tools
- Place-based approaches to reducing health inequalities
- Health equity collection
- SCIE resources on tackling inequalities in social care
- Future NHS Collaboration Platform
- NICE’s evidence standards framework for digital health technologies
- NHS Long Term Plan – chapter 2: prevention and health inequalities
- NHS Long Term Plan – menu of evidence-based interventions and approaches for addressing and reducing health inequalities
- Institute for Health Equity – resources from Professor Michael Marmot and colleagues
- Health Foundation – range of resources from organisation that promotes high-quality healthcare and equitable access
- UK Health Security Agency (UKHSA) blog - blog giving regular updates from experts on a range of subjects including health inequalities
- Health matters: public health issues collection – facts and information on public health issues
- King’s Fund – range of resources from national charitable organisation on health inequalities, population health management and other related subjects
- Department for Business, Energy and Industrial Strategy’s Industrial Strategy: the Grand Challenges
- COVID-19: understanding the impact on BAME communities
- DHSC’s Working together to improve health and social care for all white paper
- Health inequalities and the business of place-based working from the Association of Directors of Adult Social Care London and Chris Bentley
- NHS Race and Health Observatory – resources and information on the impact of race and ethnicity on people’s health
- Quality in public health – a framework for England that aims to raise quality in public health services and functions
- NHS Long Term Plan prevention priorities
- Health and Social Care Bill 2021 to 2022
- Chief Medical Officer’s annual report 2021: health in coastal communities
- Inequalities in oral health in England – report describing the current picture of oral health inequalities and oral health services inequalities in England, and ways to reduce them.