
Foreword
Teenage pregnancy prevention is a powerful example of what local leadership can achieve. Over the past two decades, councils have worked tirelessly with partners to reduce under-18 conception rates, improve outcomes for young parents, and tackle the inequalities that underpin early pregnancy.
This briefing sets out the evidence, challenges and opportunities for councils to continue leading the way. It highlights the importance of embedding high-quality relationships and sex education, ensuring access to youth-friendly contraceptive services, and supporting young people most at risk. It also highlights inspiring examples of local innovation - from targeted youth programmes to whole-system approaches that bring together education, health and community services.
As chairs of the LGA’s Health and Wellbeing Committee and Children, Young People and Families Committee, we know that teenage pregnancy prevention is not just a public health issue - it’s about safeguarding, education, social justice and giving every young person the chance to thrive. We hope this briefing supports councillors to champion this agenda in their communities and to work with partners to build on the progress made.
Councillor Wendy Taylor
Chair, LGA Health and Wellbeing Committee
Councillor Amanda Hopgood
Chair, LGA Children, Young People and Families Committee
Introduction
The focus on teenage pregnancy as a major public health issue began 25 years ago with the publication of the Teenage Pregnancy Strategy for England. A huge amount has been achieved and many lessons learned, but more needs to be done. As the LGA’s last briefing for councillors was in 2018, it seems timely to take stock of where we are, the current challenges and what more councils and their partners can do. We have produced a new briefing on supporting young parents to reach their full potential.
Recap of the Teenage Pregnancy Strategy for England
Some councillors and officers who have been involved in the 25-year journey of the strategy may remember some of the detail, but for others it’s worth a quick reminder of the key points.
Launched by the incoming Labour Government in 1999, the strategy was the first cross government initiative to address England’s historically high teenage pregnancy rates with a goal of halving the under-18 conception rate by 2010 and improving outcomes for young parents and their children. Conceptions refer to any pregnancy to a young woman under-18 whether it ends in a birth or abortion. What distinguished it from previous attempts was the decision to position teenage pregnancy as a cause and consequence of inter-generational inequality and social exclusion which required collective multi-agency action.
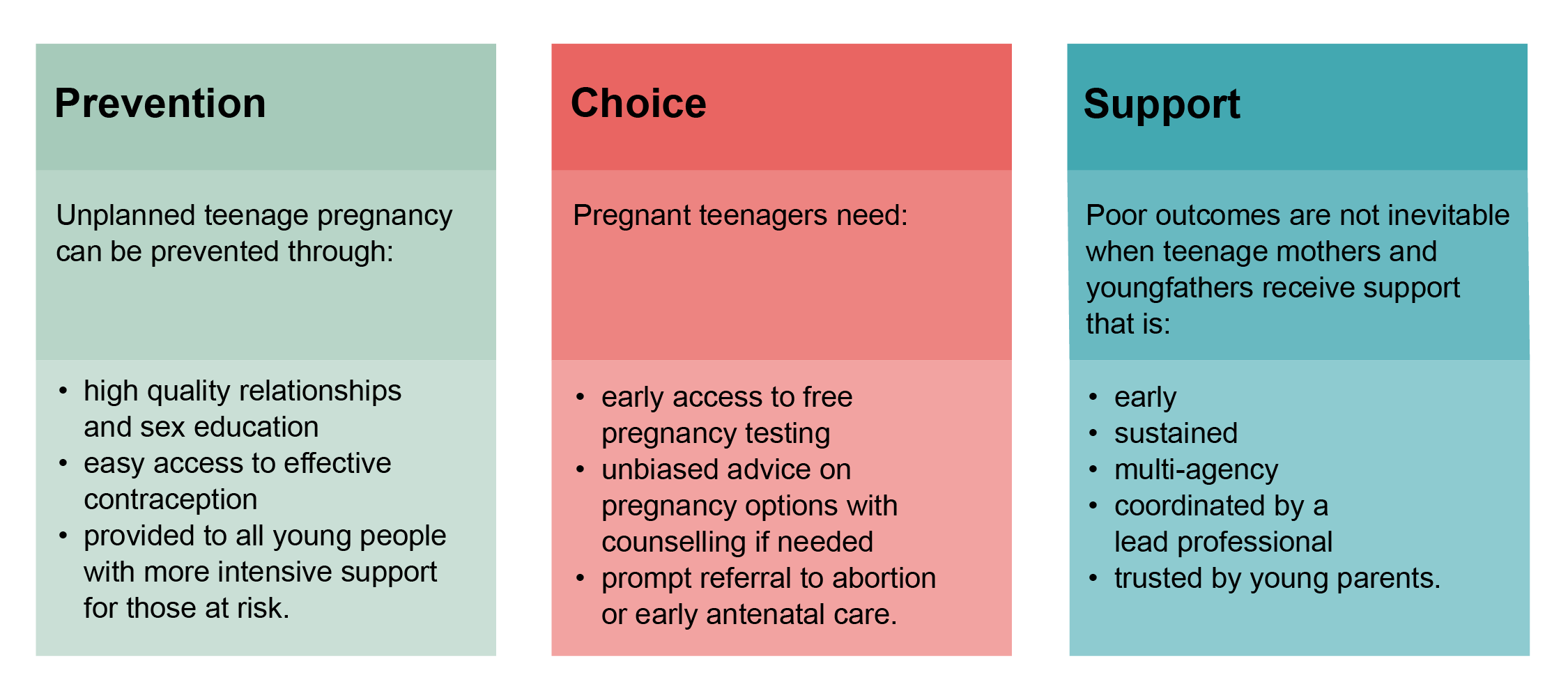
Based on international evidence, the strategy aimed to equip young people to make well informed choices about if and when they became pregnant through relationships and sex education at school, at home and in the community, and easy access to contraception. Young people who became pregnant would be given unbiased advice on pregnancy options with swift referral to their choice of abortion or maternity, and those who chose parenthood would be supported to look after their babies, return to education and fulfil their ambitions. Importantly, the strategy had a focus on inequality, with actions aimed at all young people but with more intensive support for those more at risk.
Supported by a national unit, and regional coordinators, all 150 councils agreed a 10-year reduction target, appointed a teenage pregnancy coordinator, set up a partnership board with all relevant agencies, and developed a local strategy based on national guidance.
What were the results of the strategy?
It took time for the strategy to have an impact on such a complex issue. But after 2007 progress accelerated as the cumulative actions taken by councils and their partners became embedded, and additional funding improved young people’s access to the most effective contraceptive methods. After 2010, successive governments recognised the success of the strategy asked local areas to continue to apply the lessons to make further progress, albeit with much reduced funding.
Now, 25 years on and after a huge amount of effort from councils, NHS partners, the voluntary sector and hundreds of committed individuals, the under-18 conception rate has dropped by 70 per cent, a reduction in numbers from 41,000 young women becoming pregnant in 1998, to 13,400 in 2022. There has been a similar reduction in conceptions to under-16s. Rates have dropped in all councils with a steeper decline in areas of highest deprivation.
What did we learn?
Perhaps the most important lesson from the strategy was that England’s historically high rates were not intractable. With leadership and the right actions, teenage pregnancy could be reduced, even in the most deprived areas. It is clear that if young people are equipped to make choices, they will take them.
The success factors of the strategy have been analysed with the World Health Organisation which has been sharing the lessons with other countries. Six factors stand out and remain very relevant to what happens next in England.
- Leadership by national government and local councils making clear why progress on teenage pregnancy contributes to public health, NHS, education and economic outcomes and how each agency can contribute to the solution.
- Partnership working nationally, regionally and locally – making teenage pregnancy everybody’s business.
- Embedding the strategy in wider government programmes aimed at improving youth, maternal and early years outcomes.
- Accurate data nationally and locally to monitor progress and inform commissioning.
-
Return on investment. Prevention, including early intervention to support young parents, saves money. For every £1 spent on teenage pregnancy programmes, £4 is saved.
Every £1 invested in publicly funded contraception yields a return of investment of £9 over 10 years.
- A whole system approach translates evidence into clear actions, with senior leadership at the centre.
A whole system approach: the 10 key factors for an effective programme
The below diagram shows the 10 key factors for an effective programme with strategic leadership in the centre.

Why does teenage pregnancy still matter?
Since 2018 the continued hard work of councils and their partners has maintained a downward trend, albeit at a slower rate. The 2023 ONS data publication has been delayed but the latest data for 2022 shows a small increase. While the rate remains below the pre-pandemic level, the uptick is a caution against complacency.
Conception, maternity and abortion rate per 1,000 females aged 15-17, 1998-2022
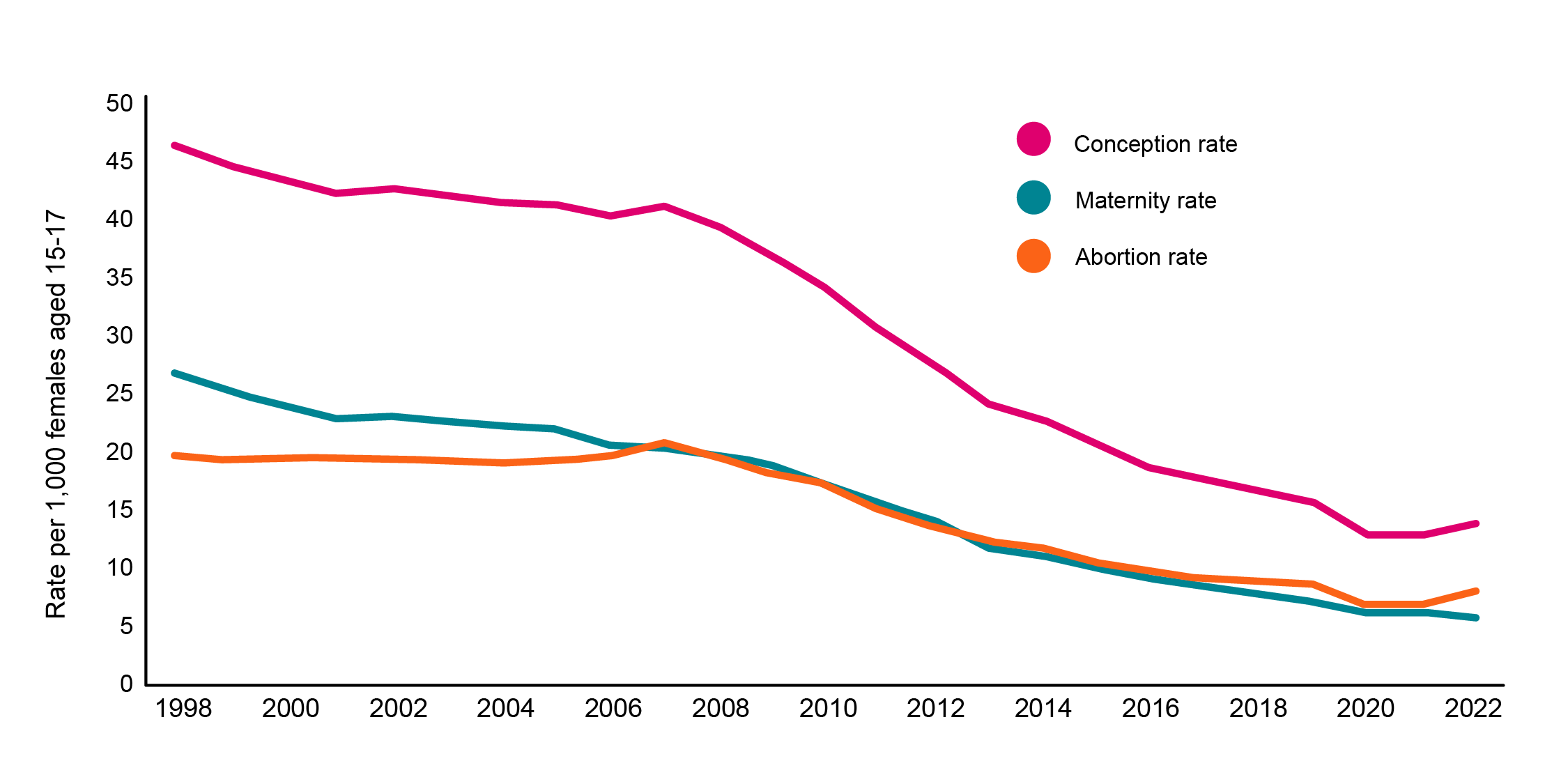
Source: Office for National Statistics (ONS)
Local and regional inequality
There is a seven-fold difference between the highest and lowest rate local areas and 60 per cent of councils have an electoral ward with a rate significantly higher than the national average.
Regional variation in under-18 conception rates 2022.
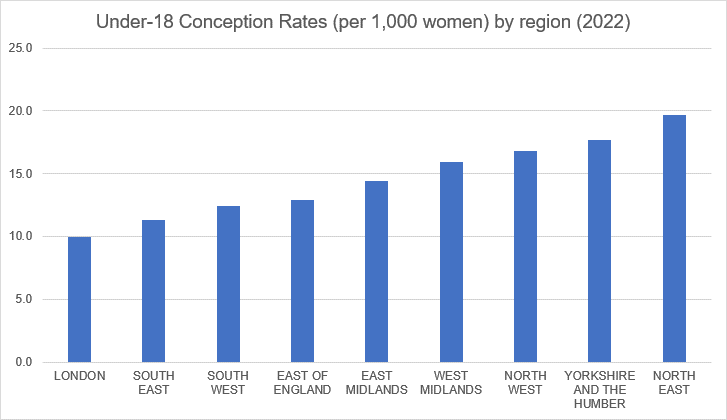
Source: Office for National Statistics (ONS)
The data is presented at regional level to support understanding of broader patterns without focusing on individual councils. A full breakdown by local authority for 2022 is available from the Office for National Statistics (ONS)
Individual inequality
Among young people, disadvantage puts some at much higher risk of early pregnancy than their peers: notably family poverty, persistent school absence, four or more adverse childhood experiences and experience of the care system. Adverse childhood experiences include; physical, sexual or emotional abuse, family breakdown, exposure to domestic violence and living in a household affected by substance misuse, mental illness or where someone has been in prison.
Individual variation
And although the number of young parents is much reduced, this smaller cohort of young mothers and fathers are entering parenthood with increased vulnerability and complex needs with resultant outcomes for them and their children disproportionately poor. The higher rates of infant mortality, maternal depression, delayed verbal ability and repeat care proceedings are a stark reminder of the impact on inter-generational inequality.
Take a look at the LGA's Supporting young parents to reach their full potential publication.
What has been the local experience of maintaining teenage pregnancy work?
To look behind the data and understand the local experience of maintaining teenage pregnancy work, recent qualitative research interviewed 16 councils to ask if any factors had made progress since 2018 more difficult. Their invaluable insights are detailed in Teenage Pregnancy and Young Parenthood: effective policy and practice.
Four concerns stood out:
Losing the priority
- A sense of complacency that the ‘rates are down, so the job is done,’ with a lack of national leadership or monitoring making it hard for local prioritisation.
The impact of austerity and cost of living crisis
- On local government and public health budgets, with funding cuts fracturing well established partnerships and upstream prevention shifting to downstream crisis management.
- On young people, some of whom have experienced an increase in the risk factors for early pregnancy - family poverty and disengagement from education, an impact clearly evidenced in the increased vulnerability of teenage parents.
The legacy of the Covid-19 pandemic
- exacerbated many of the pre-existing problems for services and young people.
- stress, long term sick leave and retirement further depleting staff numbers and weakening the fragile multi-agency partnerships.
- a large rise in numbers of pupils absent from education in years 9-11 – a key risk for early pregnancy.
Digital services and social media
- Positive innovations to simplify and increase access to contraception and sexual health services but concern about the dominance of online services jeopardising access for marginalised young people. Similar concerns were expressed about the move away from youth focused contraception and sexual health advice to all age services.
- A recognition of the potential for social media to disseminate accurate information but concerns over some types of pornography and other negative content normalising a peer culture of unhealthy and sometimes violent relationships. Social media is also influencing negative views of hormonal contraception with personal opinions of ‘influencers’ carrying more weight than health professionals.
Addressing the challenges: what next for councils in progressing teenage pregnancy work?
Faced with these challenges, council respondents showed extraordinary commitment to improving the lives of young people and were optimistic that with some national support and local system leadership further progress can be made, with four key issues to address:
- supporting schools to embed statutory relationships and sex education
- providing easy access to youth friendly contraceptive services
- ensuring RSE and contraceptive advice reaches young people most at risk
- and re-establishing and strengthening partnership working.
Embedding statutory relationships and sex education
Relationships and sex education (RSE) is learning about the emotional, social and physical aspects of human development, relationships, sexuality, wellbeing and sexual health, and has wide ranging health and safeguarding benefits.
Young people cite school RSE as their preferred source of information, and You Gov found more than nine in 10 parents support the teaching of RSE topics at school including healthy and unhealthy relationships, sexually transmitted infections and contraception.
What are the benefits of RSE for children and young people?
Independent and published research from a wide range of academic and credible sources in the UK and internationally demonstrate that Relationships and Sex Education (RSE) contributes to improved physical and mental health for children and young people.
When they have received RSE, young people are:
- more likely to seek help or speak out
- more likely to practice safe sex and have improved health outcomes
- more likely to have consented to first sex, and for first sex to happen at an older age
- more likely to have an understanding of digital safety in regard to relationships and sex
- more knowledgeable and aware of discrimination, gender equity and sexual rights
- less likely to be a victim or perpetrator of sexual violence.
And young people who reported school as their main source of RSE were less likely to have a sexually transmitted infection, a pregnancy before 18 or an unplanned pregnancy later in life.
Source: Sex Education Forum: ‘RSE the evidence’ (2022)
Statutory RSHE: A huge opportunity
The Children and Social Work Act 2017 made it mandatory for all schools in England to provide RSE, and statutory guidance on relationships, sex and health education (RSHE) was voted through in 2019 by 538 MPs. This legislative change provides a huge opportunity to lay the foundations for universal prevention and equip successive generations of children and young people with the knowledge and skills to make safe, well-informed decisions about relationships, pregnancy and sexual health.
New revised statutory guidance for schools was published in July 2025. The guidance highlights the role of RSE in helping young people prevent unplanned pregnancy and STIs and the importance of pupils knowing about local contraceptive and sexual health services.
What do young people say about school RSE?
After delays in implementation caused by the COVID-19 pandemic, the impact of statutory RSHE is starting to show. The Sex Education Forum’s Poll (2024) of 1000 16 and 17 year olds, showed a solid improvement in young people’s overall satisfaction with RSE compared to previous polls, with 50 per cent rating their RSE at school ‘good’ or ‘very good’ – 10 percentage points increase on the 2022 poll. Young people were also learning more about consent and how to tell if a relationship is healthy.
But there is much more to do to ensure the protective benefits of RSE reach all young people. The poll found RSE was reported as only ‘ok’ by 39 per cent and ‘bad’ or ‘very bad’ by 11 per cent, with several key topics not being covered sufficiently. For example, young people said they learned nothing or not enough about power imbalances in relationships (49 per cent), how to access local sexual health services (46 per cent) and STIs (35 per cent). Notably, while young people valued information, what they wanted more of in RSE lessons was open discussion and the opportunity to explore scenarios of real life examples to help them navigate the online and offline challenges of life in the 21st century.
When asked what actions from the Government would help improve RSE, young people prioritised: training for teachers; flexibility for schools to cover the RSE topics that their pupils need; and opportunities for pupils to feedback on their RSE.
How can councils help?
Evidence shows RSE is most effective when teachers (and other educators) receive evidence-based training about RSE and when home and school are involved. National government has a pivotal role in ensuring schools are equipped to deliver the highest quality RSE to their pupils, but councils play a crucial role.
Supporting schools to assess and address the needs of children and young people, engaging parents; and connecting RSE to other council priorities such as safeguarding and ending violence against women and girls. The case studies describing Surrey’s healthy schools ‘one system ambition,’ Darlington’s pupil needs assessments and Islington’s engagement with parents and the local community are three examples of the excellent work of councils across the country.
Providing young people with easy access to trusted contraceptive and sexual health services
RSE is essential in building young people’s knowledge, skills and confidence to make well informed choices about their reproductive and sexual health. But the impact on reducing unplanned pregnancy will only be achieved if councils provide all young people with easy access to contraception in youth friendly services.
The local offer may be a mix of face to face and digital services, but needs to be informed by consultation with young people, with regular monitoring to ensure it meets their needs. As the Department of Health and Social Care 'You’re Welcome' standards highlight, confidentiality, a welcoming environment and well trained youth friendly staff remain three of the most important features of a trusted service. Liverpool’s dedicated young people’s clinic, developed and branded by young people, and Barking and Dagenham’s engagement of the young inspectors programme in their condom distribution scheme both illustrate excellent local commissioning.
Investment in contraception saves money
Government analysis shows that every £1 invested in publicly funded contraception yields a return of investment of £9 over 10 years, primarily due to the prevention of unplanned pregnancies. With young people at highest risk of unplanned pregnancy and disproportionately poor outcomes for young parents and their babies, the cost effectiveness of contraceptive services is likely to be even higher
Ensuring RSE and contraceptive advice reaches young people most at risk
All young people need good RSE and access to contraception to make well informed decisions. But some young people have life experiences putting them at higher risk of pregnancy and need additional support. This may be through outreach work, taking RSE and contraceptive advice directly to young people in education or community settings, or providing training for practitioners in partner agencies to discuss relationships and sexual health and link young people into local services.
The case studies of Walsall’s targeted youth development programme, Dudley’s outreach service and Salford’s workforce training programme illustrate councils’ expertise in understanding and meeting the needs of young people most at risk.
Individual risk factors associated with pregnancy before 18:
- family poverty
- slower than expected academic progress between ages 11-14
- persistent school absence by age 14
- experience of sexual abuse and exploitation
- young person with four or more Adverse Childhood Experiences*: 3-7 times more likely to have early sex, have an accidental pregnancy or become a teenage parent by 18 and to experience a sexually transmitted infection (STI)
- care experienced young people - approximately three times rate of motherhood by the age of 18.
* Adverse Childhood Experiences: physical, sexual or emotional abuse, family breakdown, exposure to domestic violence and living in a household affected by substance misuse, mental illness or where someone has been in prison.
Re-establishing and strengthening partnership working
Partnership multi-agency working within the council and with NHS and voluntary sector partners has always been the key to effective system leadership of teenage pregnancy programmes. Weaving RSE and contraceptive advice into a diverse range of services helps to create a joined-up prevention pathway and ensure the reach to all young people, particularly those most at risk. Collaboration also harnesses the contributions other programmes make towards reducing the risk factors for early pregnancy; for example the healthy child programme, reducing school absence, supporting 16 to 18-year-olds into education or training, and improving outcomes for care experienced young people.
To enable effective commissioning, teenage pregnancy needs to sit in a strategic and sustainable partnership board. The ‘best fit’ will vary between councils. Some may retain or re-establish specific teenage pregnancy and young parent partnerships. Others will secure teenage pregnancy in a well-established board, such as Early Help or Best Start in Life.
All the case studies in this briefing reflect partnership working and its benefits. The example from Barnsley illustrates how the council relaunched the Teenage Pregnancy Prevention and Supporting Teenage Parents Partnership and used their Overview and Scrutiny process to refocus and strengthen the work on teenage pregnancy and sexual health.
A good time to review your local teenage pregnancy programme?
In the qualitative research referenced earlier, many respondents described the post-pandemic period as a window of opportunity for councils to review their teenage pregnancy programmes, re-engage partners, and harness all their local assets. They reported a strong legacy of knowledge – knowing what should be done with many committed staff still in place - with involvement of new staff in a review helping to growing the knowledge and capacity of the local system. As the case studies section show, there is much inspiring work to learn from. Walsall and Wakefield illustrate examples of councils who have reviewed and renewing their programmes and have published teenage pregnancy and young parenthood strategies for the next three to five years.
Reviewing your teenage pregnancy programme: a checklist for the 10 key factors
The questions below provide a short checklist for each of the 10 key factors. More detail and a self-assessment is provided in the Teenage Pregnancy Prevention Framework (originally PHE-LGA), which is expected to be updated later this year (2025).
Strategic leadership and accountability
- Has a teenage pregnancy lead in the council been identified, with sufficient seniority to engage partner agencies, and report directly into local governance arrangements, including the Health and Wellbeing Board?
- Where does teenage pregnancy sit within partnerships within your council? What do the other programmes of work contribute to progress on teenage pregnancy?
- Has an elected member been identified as a ‘teenage pregnancy champion’ to provide visible leadership, including with the local media?
Effective use of data for commissioning and monitoring of progress
- What is the trend in your council’s under-18 and under-16 conception rates; do you have any wards with rates significantly higher rates; what proportion of the conceptions end in abortion?
- Do you have a named lead in the council with responsibility for collation and analysis of teenage pregnancy data and local service uptake statistics?
- Do you have data sharing agreements with maternity and abortion services to provide more timely data on conceptions and identify early signs of an upward trend?
Relationships and sex education (RSE) in schools and colleges
- Do you have a dedicated lead to support schools, including special schools and alternative provision to deliver statutory RSE/RSHE; to assess pupil need, provide training and support for teachers and help schools in engagement with parents and faith communities?
- Is your RSE support connected into the council’s relevant priorities on safeguarding, parenting, prevention of violence against women and girls and sexual health, and supported to access national networks?
- Do you have clear pathways for pupils between RSE lessons and one to one confidential advice within school and college or local services, maximising the contribution of school nursing and other support service?
Youth friendly contraceptive/sexual health services and condom schemes
- Do you have a dedicated young people contraceptive and sexual health service providing the full range of contraceptive options, with digital and in person access? Is the service commissioned in line with the DHSC You’re Welcome service standards?
- Do you have a condom scheme accessible across a wide range of young person friendly venues?
- Do you monitor attendance and have arrangements for regular evaluation of the service by young people, particularly those more at risk of early pregnancy. For example through ‘mystery shopper’ initiatives, and links to Healthwatch?
Support for parents and carers to discuss relationships and sexual health
- Do you coordinate the advice and information for parents and carers on talking to their children about relationships and sexual health with family support services?
- Do you provide advice and information about reliable websites for parents on talking to children and teenagers about healthy relationships and sexual health in universal settings? For example in schools to complement RSE lessons and as part of other support to parents on pupil wellbeing?
- Do you include advice and information in other programmes and community settings supporting parents and carers – for example Early Help, Family Hubs?
Targeted prevention for young people at risk
- Does your teenage pregnancy lead collaborate with the local accountable lead for early help and intervention, to identify young people most at risk of early pregnancy and needing additional support.
- Have you considered the location of targeted prevention to engage young people at risk who may be unable or unwilling to access services. For example, those in alternative education provision or attending Youth Offending Services.
- Do you commission targeted support services which take a youth work approach, delivered in non-clinical, young people friendly settings and supporting young people on a range of issues relating to sexual health and relationship.
Training on relationships and sexual health for health and non-health professionals
- Have you Identified the agencies and practitioners who are in touch with young people, particularly those most at risk of early pregnancy. For example, Leaving Care Teams, Early Help, school attendance, NEETs, social workers?
- Do you provide training on relationships and sexual health, prioritised for agencies and practitioners working in areas with high conception rates and those working with vulnerable young people. For example, Personal Advisers, Early Help practitioners, NEETs leads, foster carers?
- Have you used the Making Every Contact Count approach of ‘Ask, Assist’ Act’ to encourage partner agencies to proactively ask young people about any sexual health and contraceptive needs and link them to services?
Advice and access to contraception in non-health, education and youth settings
- Have you reviewed contraceptive clinic attendance by young people in high rate and deprived wards to assess whether there is a need to extend provision to other settings?
- Have you identified the education and community settings used and trusted by young people where contraception and sexual health outreach could be provided– eg Further Education colleges, voluntary sector services, young futures hubs, family hubs?
- Have you established referral pathways with clinical services which offer the full range of contraception and sexual health screening and treatment if required?
Consistent messages to young people, parents and practitioners
- Do you publicise the council’s commissioned contraceptive and sexual health services to all young people in the local community through a mix of digital and other communication channels? Do you provide information about services to all secondary schools in line with the statutory RSHE guidance?
- Do you signpost young people, practitioners and parents to reliable, factually accurate information about pregnancy and sexual health?
- Do you have an arrangement for keeping relevant agencies and practitioners working with young people, informed and updated on local contraceptive and sexual health services? For example through Partnership Boards, digital newsletters and MECC?
Support for pregnant teenagers and young parents, including prevention of subsequent pregnancies
- Do you provide and publicise free pregnancy testing and easy access to unbiased pregnancy options advice?
- Do you have swift referral pathways to maternity services or abortion care and coordinated support for young parents? Take a look at the LGA councillors briefing: Supporting young parents to fulfil their potential and give their babies the best start in life.
- Do you provide information about post-pregnancy contraception during the abortion care pathway or antenatal period, and provide the chosen method at time of abortion or immediately postnatally?
Case studies
The below case studies illustrate some of the ten key factors for an effective local programme in teenage pregnancy prevention.
.